Early years (particularly birth to three years) are one of the most important periods in the life course, with experiences during this critical period laying the foundation for all future learning, health and behaviour. Due to greater neuroplasticity, early life is a sensitive window of opportunity in which the quality of the environment and experience can shape the quality of the brain development.
Adverse childhood experience during the early years can lead to neurodevelopment disruptions and impact adult outcomes including poor mental health, lower immunity and diseases including CVD and diabetes. However, not all adverse childhood experiences impact in the long term. Positive stress such as having a vaccine or going for first day of preschool is a normal adverse experience and a child can recover from it very quickly. Tolerable stress is caused by temporary adverse events buffered by supportive relationships such as grief. However, it is toxic prolonged stress such as abuse, chronic hunger, neglect and lack of services that not only impacts the learning and development but adult mental and physical health.
In this section we will present publicly available data on key infancy and early years indicators.
Child Poverty
Growing up in poverty is detrimental to children's health and well-being, affecting their future health and life chances. It is essential to provide a healthy environment for children, especially during their early years. There is a substantial body of evidence connecting adverse childhood circumstances to poor child health outcomes and future adult illness. Child poverty in England is measured by the Income deprivation affecting children index (IDACI) that measures the percentage of all children aged 0 to 15 living in income deprived families. It is a subset of the Income Deprivation Domain which measures the proportion of the population in an area experiencing deprivation relating to low income. The definition of low income used includes both those people that are out-of-work, and those that are in work but who have low earnings (and who satisfy the respective means tests).
Homelessness is another measure associated with severe poverty and is a social determinant of health. It often results from a combination of events such as relationship breakdown, debt, adverse experiences in childhood and through ill health. Homelessness is associated with poor health, education and social outcomes, particularly for children.
Income deprivation affecting children index
The latest data on income deprivation affecting children is available for the year 2019 only and therefore does not account for the impact of the pandemic. Based on this most recent data, 16.9% of children in Bury live in poverty, similar (statistically significant) to the England average of 17.1%. No trend data are available for Bury and England. Bury has the 4th lowest percentage of children living in poverty with the lowest percentage in Stockport of 14.6% and highest in St. Helens at 23.7%. Data on inequalities are only available by geography and at the Ward and MSOA levels.
Examining inequalities in IDACI by Bury wards, the highest proportion of children living in poverty are in Moorside (30.5%) and Besses (27%) and lowest in North Manor (5.8%) (Table 1)
Table 1: Child poverty (Income deprivation affecting children %) in Bury wards for the year 2019 (Local Health, 2019)

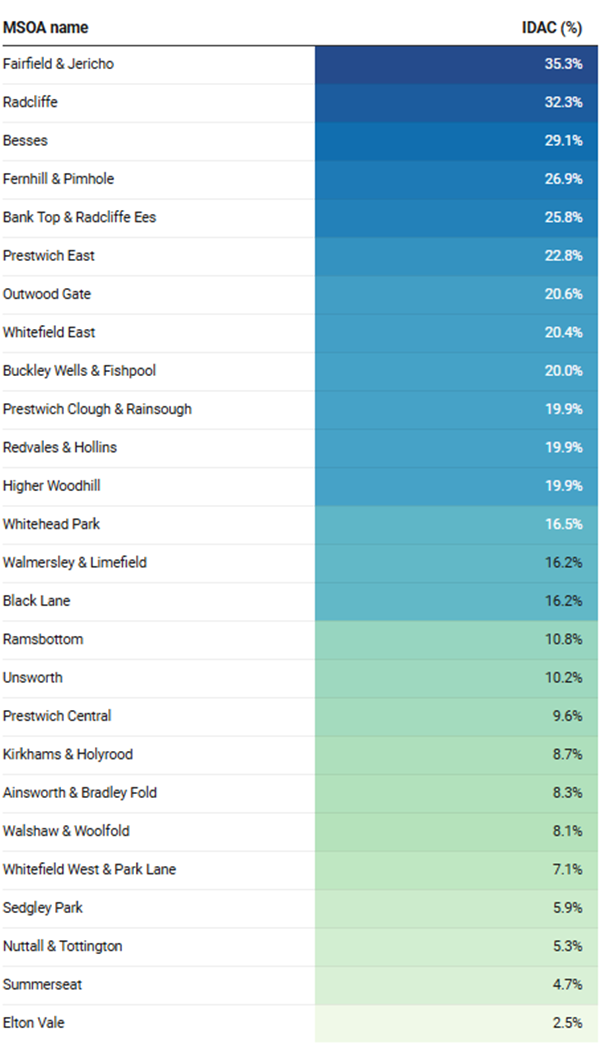
By Bury MSOAs, the highest proportion of children in poverty are in Fairfield & Jericho at 35.3% and Radcliffe at 32.3% and lowest in Summerseat at 4.7% and Kirkhams and Elton Vale at 2.5% (Table 2).
Table 2: Child poverty (Income deprivation affecting children %) in Bury MSOAs for the year 2019 (Local Health, 2019)
Homelessness - households with dependent children owed a duty under the Homelessness Reduction Act
This indicator is defined as ‘Households including one or more dependent children owed a prevention or relief duty under the Homelessness Reduction Act, crude rate per 1,000 estimated households that include at least one dependent child. Children should count as dependent if they're under 18 and living at home.’ It is included in this section as it covers the age range 0-5 years.
Homelessness in Bury for the period 2022/23 is 14.3 per 1,000 household, statistically lower than England average of 16.1 and lower than NW average of 17.7 (Child and Maternal Health Profile, 2023).
Amongst Bury’s group of 6 statistical children service neighbours, Bury has the second highest rate, with the highest rate in Stockton-on-Tees at 27.3 and lowest in Sefton at 7.5 (Child and Maternal Health Profile, 2023).
There are no data on inequalities for Bury and England.
Infant Mortality
Infant mortality is an indicator of the general health of population reflecting both the availability and quality of healthcare services as well as broader social and economic and environmental factors. It is measured as number of deaths of infants under one year of age per 1,000 live births. Infant mortality rate can be split by neonatal deaths (under 28 days) and post-neonatal deaths (between 28 days and 1 year). Over the past 40 years, infant mortality rates have significantly declined across the UK countries. However, compared to other European countries, development has slowed over the past twenty years.
Some infant deaths can be prevented by targeting interventions to reduce the modifiable risk factors that occur in around a third of infant deaths. These factors have a multiplier effect where greater number of these factors can make the infant more vulnerable. The most common modifiable risk factors are smoking in pregnancy, obesity in pregnancy and household smoking. In addition to these, there are protective factors that can reduce infant mortality and include vaccinations (including flu vaccination for pregnant women), breastfeeding, and safe-sleeping practices.
The infant mortality rate for Bury is 6.2 per 1000 live births and is statistically worse compared to England average of 4.1 per 1000 live births (Child and Maternal Health Profile, 2023).
Figure 1: Trend in infant mortality in Bury from the period 2001-2003 to 2021-23

Neonatal mortality (deaths under 28 days per 1000 live births) is 4.5 for Bury, higher and statistically worse than the England average of 3 per 1000 live births (Child and Maternal Health Profile, 2023). Since the period 2010-12, Bury had the highest number of neonatal deaths (28) in the period 2021-23. Post neonatal mortality rate for Bury is 1.6 per 1000 live births is statistically similar to England average of 1.1 (Child and Maternal Health Profile, 2023). Due to small numbers, this could be due to random year-to-year fluctuations. Figure 2 below presents the trend in infant mortality by neonatal and post-neonatal mortality in Bury, and we can see that deaths under 28 days (neonatal mortality) makes the highest contribution to the infant mortality rates in Bury.
Figure 2: Trend in infant mortality by neonatal and post-neonatal mortality in Bury from the period 2010-12 to 2020-22

There is currently no national target for the infant mortality rate in England but the government has a national ambition in England to achieve 50% reductions in neonatal mortality by 2030. The lack of data at local level means it is not possible to examine inequalities with the exception of sex for neonatal mortality, but data for England suggests local inequalities by deprivation and ethnicity, where deprived areas, black ethnic groups and Asian ethnic groups see higher infant mortality rates (Nuffield Trust, 2022). Data for Bury by sex suggests higher neonatal mortality rates for males (3.2 per 1000 live births) compared with females (2.6 per 1000 live births). Although neonatal mortality is generally 20% higher in boys than girls due to biological phenomena, research suggests that socioeconomic factors such as income and education are associated with these differences in neonatal mortality rates between males and females (Kramer et al, 2002).
Health Visitor Reviews
All children should be evaluated by a team led by a health visitor shortly before their first birthday. This allows for an assessment of the baby's physical, emotional, and social needs within the context of their family, including predictive risk factors and allows both parents to discuss any concerns they may have about their baby's health, as well as a reminder of the importance of vaccinations at around one year. It also allows for growth monitoring and discussions about weaning, oral health, and home safety (particularly relevant as babies are now sitting independently, rolling over, and may be starting to walk). Furthermore, it provides an opportunity to discuss preconception health prior to any future pregnancy. A review every 9 to 12 months ensures that any issues are identified early and appropriate referrals are made.
New Birth Visits
All infants and their families are eligible to receive a visit led by a health visitor within the first two weeks from birth, which is known as the New Birth Visit (NBV). This metric is designed to measure what proportion of infants receive a timely NBV. This visit forms part of the Healthy Child Programme (HCP) and is important to ensure a continuum of support following on from visits by a midwife, which usually end at day 10. This visit is also important in identifying any development issues with the infant (including early referral to a specialist team where needed), to promote sensitive parenting, to provide safe sleeping advice, to support feeding and to discuss concerns and worries, including maternal mental health (Child and Maternal Health Profiles, 2024).
Proportion of New Birth Visits completed within 14 days in Bury for the year 2023/24 was 33.7%, statistically worse than England average of 83%. Data for Bury has been inconsistently reported but trend data based on the five most recent data points suggests a decreasing and worsening trend (Figure 3).
Figure 3: Proportion of New Birth Visits completed within 14 days (%) 2017/18 to 2023/24 for Bury and England (Child and Maternal Health Profiles, 2024)
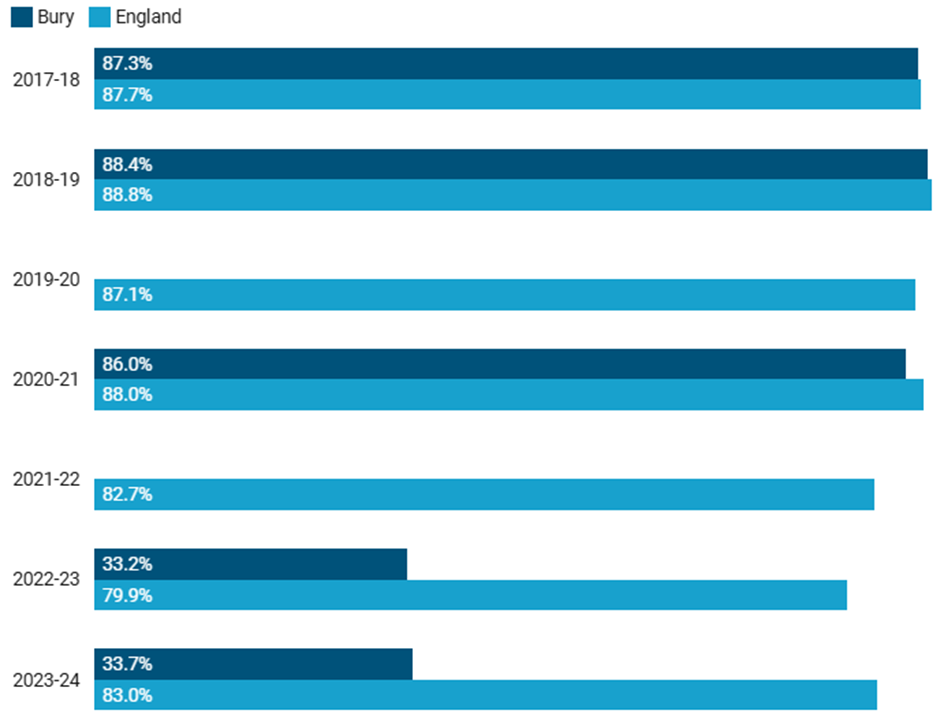
Bury has the lowest proportion of NBV being completed within 14 days when compared to its’ statistical neighbours, with the highest proportion being in Derby at 98% for 2023/24 (Child and Maternal Health Profiles, 2024). There are no available data on inequalities at the Bury level. However, national-level data for 2023/24 suggests an inverse deprivation gradient with higher proportion of New Birth Visits (NBVs) completed within 14 days in areas with greater deprivation. In the most deprived decile, 85.5% of NBVs were completed within 14 days compared to 76.3% in the least deprived decile. (Child and Maternal Health Profiles, 2024).
6–8-week review
The 6-to-8-week review is an opportunity for support with breastfeeding if required and allows an assessment of the mother’s mental health, as well as reinforcing the discussions and messages from the new birth visit. It is an opportunity to ensure the mother has had a six-week postnatal check and that the infant has received the infant physical examination, as well as a reminder of the importance of the vaccinations that take place in the first few months. Any difficulties the mother has had in receiving benefits she is entitled to can be discussed and support offered (Child and Maternal Health Profiles, 2024).
The proportion of infants receiving 6–8-week review in Bury for the year 2023/24 was 72.2%, significantly worse than England average of 81.8%. The trend in Bury is decreasing and getting worse based on the 5 most recent data points, reducing from 78.1% in 2017/18 to 72.2% in 2023/24 (Figure 4). Although the rate in England has also declined from 84.3% in 2017/18 to 81.8% in 2023/24, it remains significantly higher than the proportion in Bury.
Figure 4: Proportion of infants receiving a 6-8 week review (%) 2017/18 to 2023/24 for Bury and England (Child and Maternal Health Profiles, 2024)
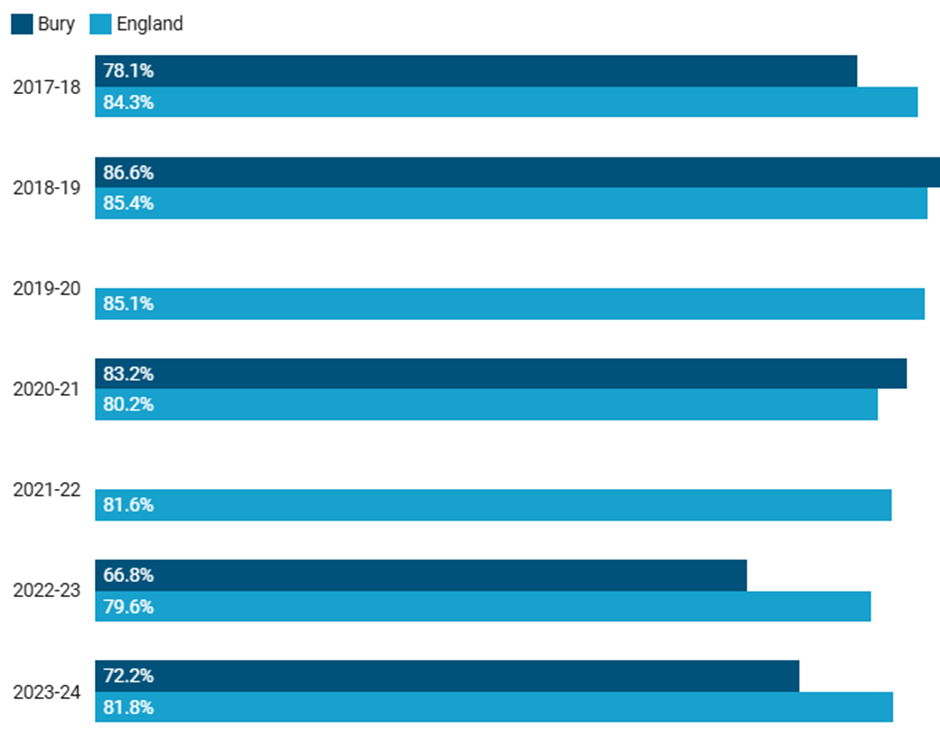
Bury has the second lowest proportion of infants receiving a 6-8 week review when compared to its’ statistical neighbours for 2023/24, with the lowest proportion being in Kirklees (70.1%) and the highest in Wigan (97.3%) (Child and Maternal Health Profiles, 2024). Data on inequalities are unavailable at Bury level and national data do not show a deprivation gradient (Child and Maternal Health Profiles, 2024).
12-month review
All children should receive a review by a health visitor led team shortly before they turn one year. This allows for assessment of the baby’s physical, emotional and social needs in the context of their family, including predictive risk factors and provides an opportunity for both parents to talk about any concerns that they may have about their baby’s health, as well as a reminder of the importance of the vaccinations at around one year. It also allows monitoring of the baby’s growth and discussions on weaning, oral health and home safety (particularly relevant as babies are now sitting independently, rolling over and may be starting to walk). In addition, it presents an opportunity to discuss preconception health before any future pregnancy. A review between 9 and 12 months ensures any issues can be identified early and referrals made as appropriate. However, it is accepted that for many reasons these reviews may be a little late and the content is still of value. This metric therefore shows the proportion of children who have a 12-month review on time or slightly late (by 15 months) (Child and Maternal Health Profiles, 2024).
Proportion of infants receiving a 12-month review for the year 2023/24 was 77.1%. Despite Bury initially having a higher proportion (statistically significant) of children receiving a 12-month review in 2017/18 (97.8%) when compared to England (82.6%), it has decreased over time to 77.1% in 2023/24 and is now lower (statistically significant) than the average for England (86.5%). There have been inconsistencies in data available for Bury for this measure, however the available data shows a decreasing trend (based on five most recent data points) with only just over three quarters of children receiving a 12-month review for the latest time period (Figure 5).
Figure 5: Proportion of infants receiving a 12-month review (%) 2017/18 to 2023/24 for Bury and England (Child and Maternal Health Profiles, 2024)
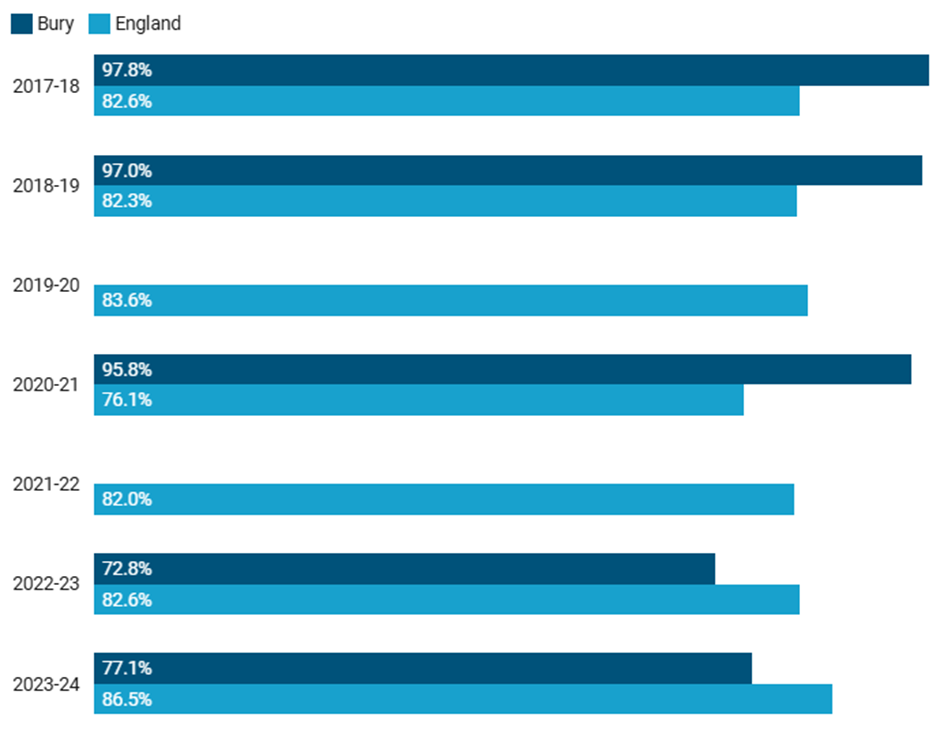
Bury has the lowest proportion of infants receiving a 12-month review when compared to its’ statistical neighbours for 2023/24 and is the only local authority in its group that is worse (statistically significant) compared to England average, with the highest proportion being in Sefton at 97.5% (Child and Maternal Health Profiles, 2024). Data on inequalities are unavailable at a Bury level but the data at national level suggests that the more deprived the area, the higher the proportion of 12-month reviews being completed, with the most deprived decile having 89.9% of reviews completed, compared to 81.7% in the least deprived decile for 2023/24 (Child and Maternal Health Profiles, 2024).
2 to 2½ year review
All children and families should receive a review when the child reaches around 2 to 2 1/2 years. This allows for an integrated review of their health and development. In addition, it presents an opportunity to discuss preconception health with parents before any future pregnancy, an opportunity to support the parents with issues such as access to a nursery place (including free provision) and a reminder of the importance of the pre-school immunisation booster (Child and Maternal Health Profiles, 2024).
Proportion of infants receiving a 2 to 2½ years review for the year 2023/24 was 62.1%. Despite Bury initially having a higher proportion (statistically significant) of children receiving a 2 to 2½ years review in 2017/18 (90.7%) when compared to England (75.7%), it has decreased over time to 62.1% in 2023/24 and is now lower (statistically significant) than the average for England (78.4%). There have been inconsistencies in data available for Bury for this measure, however the available data shows a decreasing trend (based on five most recent data points) (Figure 6).
Figure 6: Proportion of infants receiving a 2 to 2½ years review (%) 2017/18 to 2023/24 for Bury and England (Child and Maternal Health Profiles, 2024)
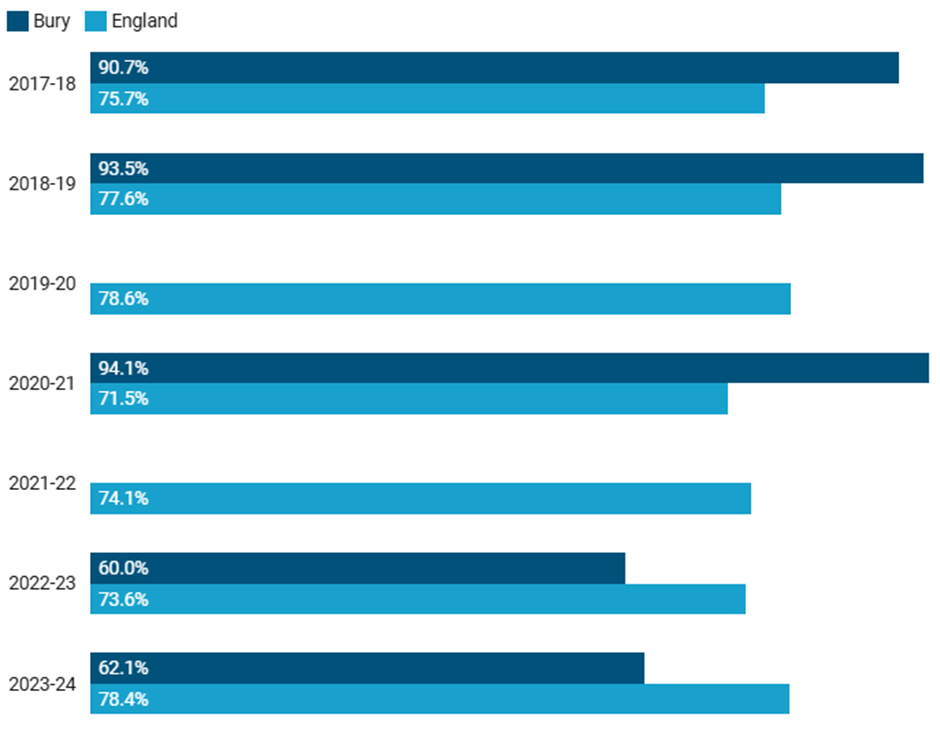
Bury has the lowest proportion of infants receiving a 2 to 2½ years review when compared to its statistical neighbours for 2023/24, with the highest proportion in Sefton at 92.2% (Child and Maternal Health Profiles, 2024). Data on inequalities are unavailable at Bury level but data at the national level suggests that the more deprived deciles have a higher percentage of infants receiving a 2 to 2½ years review for 2023/24, as 83.9% received a review in the most deprived decile compared to 71.1% in the least deprived decile (Child and Maternal Health Profiles, 2024).
Immunisation Coverage
After clean water, vaccination is the most effective public health intervention in the world for saving lives and promoting good health. Immunisation is a triumph of global health and development, saving millions of lives annually. Vaccines reduce the likelihood of contracting a disease by bolstering the body's natural defences. Immunisation is an essential aspect of primary health care and an indisputable human right (WHO, 2019). In addition to reducing infectious disease mortality and morbidity, vaccines have other beneficial impacts on health, the economy and our society. Vaccines induce herd immunity, reduce diseases that complicate vaccine preventable diseases and prevent antibiotic resistance. They also lead to significant cost savings and a return on investment of £34. Societal impact of the vaccines includes empowering women, strengthening health and social care infrastructure and improving life expectancy and opportunities for a healthy life.
United Kingdom has one of the best immunisation programmes in the world that has always been at the forefront of rolling out new programmes when the best vaccination is available. The UK childhood immunisation programme provides protection against 14 childhood infections including polio, mumps, measles, meningococcal diseases and rubella. The programme is divided into routine (Table 3) and selective childhood immunisation programmes (Table 4).
Table 3: Routine childhood immunisations offered to children under 5 years of age in the UK (HM Government, 2022)

Table 4: Selective childhood immunisations offered to children under 5 years of age in the UK (HM Government, 2022)

Immunisation coverage is the best indicator of the level of protection a population will have against vaccine preventable communicable diseases. Coverage is closely correlated with levels of disease. Monitoring coverage identifies possible drops in immunity before levels of disease rise.
This section will present publicly available immunisation data on vaccinations given to children until 5 years of age.
BCG Immunisation
BCG immunisation programme is part of selective childhood immunisation and is a risk-based programme. BCG vaccine is offered to all infants (0 to 12 months old) living in areas where the incidence of tuberculosis is greater than 40 per 100,000 or where a parent or grandparents is born in a high incidence country. The vaccine is given when a baby is around 28 days old. Three-year average incidence of TB in Bury is 6 per 100,000 population (2021-23), so there is no universal programme in the Borough and babies with parents and grandparents born in a high incidence country are being offered the vaccine. Count data for Bury are only available for children for whom the local authority is responsible receiving a dose of BCG vaccine at any time by their first birthday. For the year 2023/24, 428 babies were given the BCG vaccine by the age of 3 months in Bury.
Population vaccination coverage: Dtap IPV Hib HepB
The combined Dtap IPV Hib HepB is the first in a course of vaccines offered to babies to protect them against diphtheria, pertussis (whooping cough), tetanus, Haemophilus influenzae type b (an important cause of childhood meningitis and pneumonia) and polio (IPV is inactivated polio vaccine).
Dtap IPV Hib HepB (1 year old)
The coverage is measured as ‘children for whom the local authority is responsible who received 3 doses of DTaP IPV Hib HepB vaccine at any time by their first birthday as a percentage of all children whose first birthday falls within the time period.’
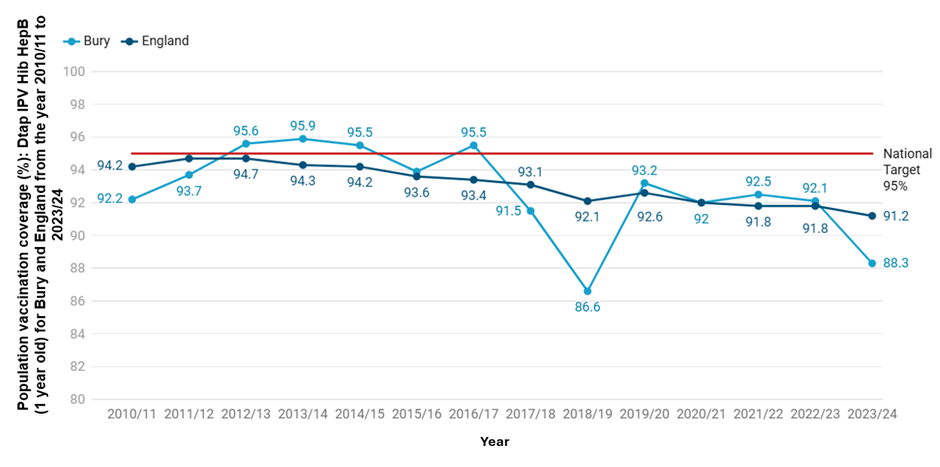
The combined DTaP IPV Hib HepB coverage (1 year old) in Bury for the year 2023/24 was at 88.3%, lower than the North West (NW) average of 90% and lower (statistically significant) than the England average of 91.2%. Coverage in Bury remains below the national target of 95%. To meet this target, 140 additional children would need to be vaccinated.
In Bury, vaccine coverage for one-year-olds has varied over time, ranging from a low of 86.6% in 2018/19 to a peak of 95.9% in 2013/14. The trend initially showed steady improvement, rising from 92.2% in 2010/11 to above the national target of 95% in 2012/13, when coverage reached 95.6%. This was followed by a decline to 93.9% in 2015/16, then a brief recovery to 95.5% in 2016/17. However, coverage dropped again, reaching its lowest point of 86.6% in 2018/19. It then increased to 93.2% in 2019/20, and remained relatively stable, with 92.1% recorded in 2022/23. A further decline was observed in 2023/24, with coverage falling to 88.3%. Based on the five most recent data points, the coverage in Bury is decreasing and getting worse. Nationally, vaccine coverage in England has also declined steadily, from 94.2% in 2010/11 to 91.2% in 2023/24 (Figure 7).
Figure 7: Dtap IPV Hib HepB (1 year old) vaccination coverage for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)
Bury has the lowest Dtap IPV Hib HepB (1 year old) in its group of 6 statistical children service neighbours for 2023/24, with the highest percentage in Stockton-on Tees at 95.5% (Children and Maternal Health, 2024). There are no data on inequalities at Bury level but England data suggests decreasing coverage of Dtap IPV Hib HepB vaccination with increasing levels of deprivation. The most deprived decile in England has a coverage of 87% compared with 93.8% in the least deprived decile for the year 2023/24 (Child and Maternal Health, 2024).
Dtap IPV Hib HepB (2 years old)
This indicator is defined as ‘Children for whom the local authority is responsible who received 3 doses of DTaP IPV Hib HepB vaccine at any time by their second birthday as a percentage of all children whose second birthday falls within the time period.’
The combined DTaP IPV Hib HepB coverage (2 years old) in Bury for 2023/24 was 91.8%, the same as the North West (NW) average of 91.8% and statistically similar to England average of 92.4%. Although statistically similar to the percentage in England, the coverage is still below the target of 95% and over. Bury needs to vaccinate 73 additional children to reach the national target.
Vaccine coverage for two-year-olds in Bury has ranged from a low of 91.7% in 2018/19 to a high of 96.8% in 2012/13. Coverage steadily increased from 95.8% in 2010/11 to 96.8% in 2012/13 and then remained relatively stable with minor fluctuations until 2016/17, when it stood at 96.3%. A sharp decline followed, with coverage dropping to 92.5% in 2017/18 and further to 91.7% in 2018/19. This was followed by a gradual recovery, rising to 92.6% in 2019/20 and reaching 93.9% in 2021/22. However, the subsequent years saw a slight decline, with coverage falling to 93.8% in 2022/23 and 91.8% in 2023/24.
Since 2016/17, DTaP/IPV/Hib/HepB vaccination coverage for two-year-olds in Bury has remained below the national target of 95%. Based on the five most recent data points, there is no statistically significant trend in Bury. Coverage in England has steadily declined from 96% in 2010/11 to 92.4% in 2023/24 (Figure 8).
Figure 8: Dtap IPV Hib HepB (2 years old) vaccination coverage for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Bury has the third lowest Dtap IPV Hib HepB (2 years old) in its group of 6 statistical children service neighbours, with the lowest percentage in Sefton at 91.3% and highest in Stockton-on-Tees at 95% (Children and Maternal Health, 2024). There are no data on inequalities at Bury level but England data suggests decreasing coverage of Dtap IPV Hib HepB vaccination with increasing levels of deprivation. The most deprived decile in England has a coverage of 89.3% compared with 94.2% in the least deprived decile for the year 2023/24 (Child and Maternal Health, 2024).
Geographical variations in Dtap IPV Hib HepB vaccination in Bury
Data on geographical inequalities are not available for coverage at 1 years but available at the Primary Care Network (PCN) and GP practice levels only for babies who received at least 3 doses of a DTaP vaccine before the age of 8 months and for those who received it at any time by their second birthday. We will be presenting data at PCN levels only. Bury has four PCNs: Bury PCN, Horizon PCN, Prestwich PCN and Whitefield District and Community PCN. Data at GP levels are available here.
· Coverage by PCN for Dtap IPV Hib HepB (8 months old)
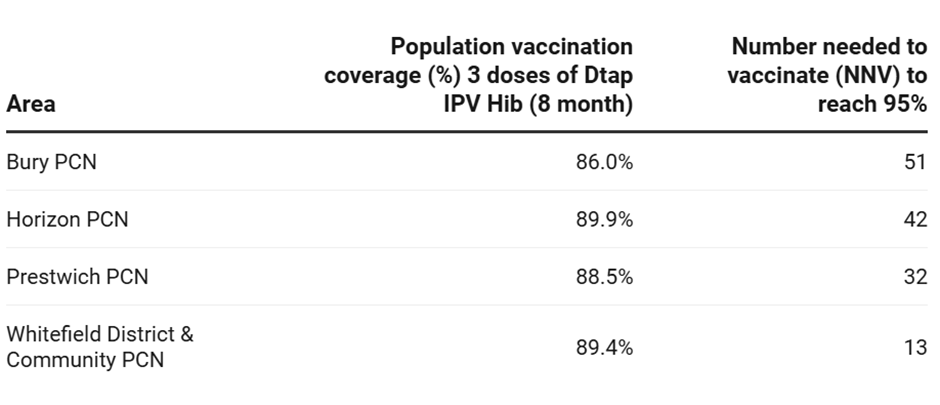
All 4 of Bury PCNS are below the national target of coverage 95% and over, for the latest time period of 2023/24. The lowest coverage is in Bury PCN at 86% and highest in Horizon PCN at 89.9%. Bury PCN has the highest number of babies (51) needed to vaccinate and Whitefield District and Community PCN has the lowest number of babies (13) to vaccinate to reach national target of 95% (Table 5).
Table 5: Vaccination coverage (%) for babies receiving at least 3 doses of a DTaP vaccine before the age of 8 months and number needed to vaccinate (NNV) to reach national target of 95% across Primary Care Networks in Bury 2023/24 (National General Practices Profile, 2024)
· Coverage by PCN for Dtap IPV Hib HepB (2 years old)
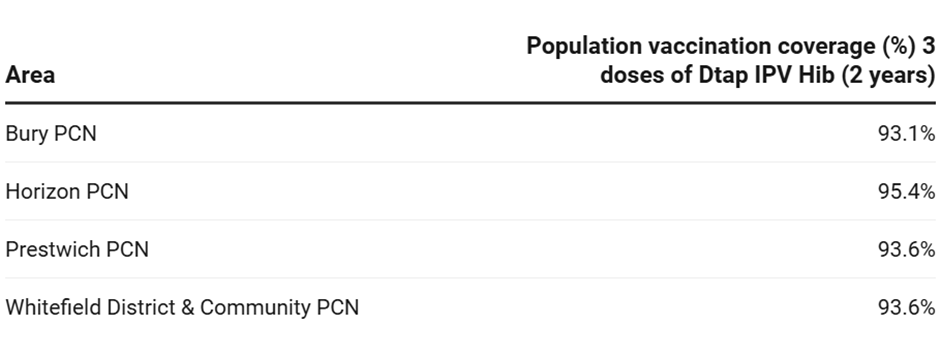
Horizon PCN is the only PCN in Bury with coverage above 95% at 95.4% for 2021/22. The lowest coverage is in Bury PCN at 93.1%. There are no figures available for the number needed to vaccinate to reach the national target of 95%.
Table 6: Vaccination coverage (%) for children receiving at least 3 doses of a DTaP vaccine at any time by their second birthday in Bury (National General Practices Profile, 2024)
Population vaccination coverage: Mumps, Measles and Rubella (MMR)
The MMR vaccine provides protection against measles, mumps, and rubella. Measles, rubella, and mumps are highly contagious diseases that can cause serious complications, such as meningitis, encephalitis, and deafness. They can also cause pregnancy complications that affect the unborn child and can result in a miscarriage. To achieve herd immunity from measles, a population vaccination coverage of 95% is required.
Children receive their first MMR vaccination as part of the routine immunisation schedule, typically within a month of their first birthday. They will then receive a booster dose before starting school, which typically occurs between the ages of three and five (Table 3 above).
Mumps, Measles and Rubella (MMR) one dose at 2 years old
This indicator is defined as ‘all children for whom the local authority is responsible who received one dose of MMR on or after their first birthday and at any time up to their second birthday as a percentage of all children whose second birthday falls within the time period.’
Mumps, Measles and Rubella (MMR) one dose coverage in (2 years old) in Bury for the year 2023/24 was at 85.7%, lower than the North West (NW) average of 88.6% and the England average of 88.9%. The coverage is still below the target of 95% and worse (statistically significant) than England average. Bury needs to vaccinate 5,281 additional children to reach the national target.
Vaccine coverage in Bury ranged from the lowest at 85.7% in 2023/24 to the highest coverage at 95.3% in 2012/13. Examining the trend in Bury, the coverage steadily increased from 89.7% in 2010/11 to 95.3% in 2012/13 and then steadily declined to 90.4% in 2016/17. This was followed by slight fluctuations but an overall increase to 94.4% in 2019/20. Following this, coverage in Bury declined to 91.2% in 2020/21 and 91% in 2021/22, followed by two further periods of decline to 89.1% in 2022/23 and finally to its lowest at 85.7% in 2023/24. After the year 2013/14, vaccination coverage of Mumps, Measles and Rubella (MMR) one dose coverage (1 year old) has remained below the national target of 95% and over. Based on the five most recent data points, trend in Bury is decreasing and getting worse. Coverage in England has fluctuated, increasing from 89.1% in 2010/11 to 92.7% in 2013/14. This was followed by a steady decline from 92.3% in 2014/15 to 89.2% in 2021/22, followed by an increase to 89.3% in 2022/23 then a slight decrease to 88.9% in 2023/24 (Figure 9).
Figure 9: MMR one dose (2 years old) vaccination coverage for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Bury has the lowest MMR one dose coverage (2 years old) in its group of 6 statistical children service neighbours for 2023/24, with the highest percentage in Stockton-on-Tees at 93.3% (Children and Maternal Health, 2024). There are no data on inequalities at Bury level but England data suggests decreasing coverage of MMR one dose coverage (2 years old) with increasing levels of deprivation. The most deprived decile in England has a coverage of 89.3% compared with 94.2% in the least deprived decile for the year 2023/24 (Child and Maternal Health, 2024).
Mumps, Measles and Rubella (MMR) one dose at 5 years old
This indicator is defined as ‘All children for whom the local authority is responsible who received one dose of MMR on or after their first birthday and at any time up to their fifth birthday as a percentage of all children whose fifth birthday falls within the time period’.
Mumps, Measles and Rubella (MMR) one dose coverage (5 years old) in Bury for the year 2023/24 was 93.2%, slightly higher than North-West (NW) average of 93% and England average of 91.9%. However, the coverage is still below the target of 95% and over but statistically similar to England average. Bury needs to vaccinate 45 additional children to reach the national target.
Vaccine coverage in Bury ranged from the lowest at 93.2% in 2023/24 to the highest coverage at 97.1% in 2015/16. Examining the trend in Bury, the coverage steadily increased from 93.6% in 2010/11 to 97.1% in 2015/16 and then declined to 95.5% in 2016/17. Coverage then remained steady with slight fluctuations until 2020/21 (96%) before sharply declining to below national target (94.8%) in 2021/22. This has been followed by two further periods of decline to 93.7% in 2022/23 and then to 93.2% in 2023/24. After the year 2010/11, 2021/22 is the first year that Bury’s MMR vaccination coverage for one dose at 2 years has declined below the national target and remains below this. Trend data based on the five most recent data points suggests that vaccine coverage in Bury is decreasing and getting worse. Coverage in England has fluctuated, increasing from 91.9% in 2010/11 to 95% in 2016/17. This was followed by a steady decline from 94.9% in 2017/18 to 91.9% in 2023/24 (Figure 10).
Figure 10: MMR one dose (5 years old) vaccination coverage for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Bury has the second lowest MMR one dose coverage (5 years old) in its group of six statistical children service neighbours for 2023/24, with the lowest percentage in Sefton at 92.4% and highest in Stockport at 95.6% (Children and Maternal Health, 2024). There are no data on inequalities at Bury level but England data suggests decreasing coverage of MMR one dose coverage (5 years old) with increasing levels of deprivation. The most deprived decile in England has a coverage of 89.4% compared with 93.8% in the least deprived decile for the year 2023/24 (Child and Maternal Health, 2024).
Mumps, Measles and Rubella (MMR) two doses at 5 years old
This indicator is defined as ‘All children for whom the local authority is responsible who received two doses of MMR on or after their first birthday and at any time up to their fifth birthday as a percentage of all children whose fifth birthday falls within the time period.’
Mumps, Measles and Rubella (MMR) two doses coverage (5 years old) in Bury for the year 2023/24 is at 81.5%, lower than both the North West (NW) average of 84.5% and the England average of 83.9%. The coverage in Bury is below the target of 95% and over and is worse (statistically significant) than the England average. Bury needs to vaccinate 335 additional children to reach the national target.
Vaccine coverage in Bury steadily increased from 82.5% in 2010/11 to the highest coverage at 93.8% in 2014/15. The coverage steadily declined from 92.7% in 2015/16 to 88.3% in 2017/18 and then remained fairly stable until 2020/21 with a coverage of 89%. In the year 2021/22, coverage in Bury declined to 87.3%, followed by two further periods of decline to 83.3% in 2022/23 and then to its lowest level of 81.5% for 2023/24. Based on the five most recent data points, trend data suggests that coverage in Bury is decreasing and getting worse.
Examining trend data for England, coverage in England steadily increased from 84.2% in 2010/11 to 88.6% in 2014/15. This was followed by a steady decline from 88.2% in 2015/16 to 83.9% in 2023/24. Throughout the 11 year period, vaccination coverage for 3 doses of MMR (5 years old) remained below the national target of 95% for both Bury and England (Figure 11).
Figure 11: MMR two dose (5 years old) vaccination coverage for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Bury has the lowest MMR two dose coverage (5 years old) in its group of six statistical children service neighbours, with the highest percentage in Stockport at 90.4% for the year 2023/24 (Children and Maternal Health, 2024). There are no data on inequalities at Bury level but England data suggests decreasing coverage of MMR two dose coverage (5 years old) with increasing levels of deprivation. The most deprived decile in England has a coverage of 78.1% compared with 88.6% in the second least deprived decile and 86.9% in the least deprived decile for the year 2023/24 (Child and Maternal Health, 2024).
Geographical variations in MMR vaccination
Data on geographical inequalities are only available for MMR vaccine for one dose at 2 years old at Primary Care Network (PCN) and GP practice levels. We will be presenting data at PCN levels only. Data at GP levels are available here.
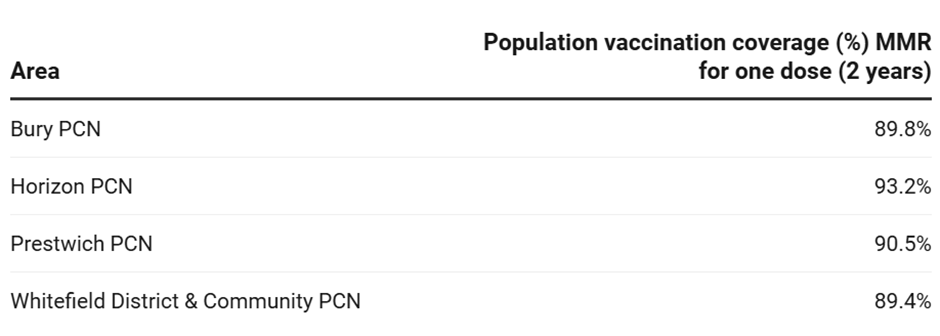
· Coverage by PCN for one dose (2 years)
All 4 of Bury PCNS are below the national target of coverage 95% and over for 2021/22. The lowest coverage is in Whitefield District and Community PCN at 89.4% and the highest in Horizon PCN at 93.2%. There are no available data on the numbers of children needed to vaccinate in order to reach the national target of 95% across primary care networks (Table 7).
Table 7: Vaccination coverage (%) for children receiving MMR vaccination for one dose (2 years) and number needed to vaccinate (NNV) to reach national target of 95% across primary care networks in Bury in 2021/22 (National General Practices Profile, 2022)
Population vaccination coverage: Hib and MenC booster
The Hib and MenC booster increases the protection provided by the initial course of Hib vaccine administered at 8, 12 and 16 weeks of age, and the MenC vaccine administered at 12 and 16 weeks of age. This enhanced immunity is maintained into adulthood.
This indicator is defined as ‘Children for whom the local authority is responsible who received a booster dose of Haemophilus influenzae type b (Hib) and Meningococcal group C (MenC) vaccine at any time by their second birthday as a percentage of all children whose second birthday falls within the time period.’
For the year 2023/24, vaccination coverage of the Hib and MenC booster in Bury was 84.5%, lower than both the North West (NW) average of 88.2% and England average of 88.6%. The coverage in Bury is below the target of 95% and over and worse (statistically significant) than England average. Bury needs to vaccinate 240 additional children to reach the national target.
Vaccine coverage in Bury steadily increased from 90.9% in 2010/11 to the highest coverage at 93.2% in 2014/15. The coverage then declined to 89.5% in 2016/17. This was followed by an increase in coverage to 91.5% in 2017/18, followed by fluctuations that continued until 2019/20, where the coverage was 93.9%. Coverage has since declined to 90.7% in 2020/21 and 90.4% in 2021/22, then further declined to 88.7% in 2022/23 and to its lowest at 84.5% in 2023/24. Trend data for Bury suggests that the coverage is declining and getting worse (statistically significant). Throughout the 11 year period, vaccination coverage for 3 doses of MMR (5 years old) for both Bury and England remained below the national target of 95% (Figure 12).
Figure 12: Trend in population vaccination coverage Hib and MenC booster (2 years old) for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Bury has the lowest population vaccination coverage Hib and MenC booster in its group of six statistical children service neighbours for 2023/24, with the highest percentage in Stockton-on-Tees at 93.1% (Children and Maternal Health, 2024). There are no data on inequalities at Bury level, but data at England level suggests a decrease in vaccination coverage as the deprivation level increases. For example, vaccination coverage for Hib and MenC booster for 2 year olds for the most deprived decile was 83.7% for 2023/24, compared to 92.1% in the second least deprived decile and 90.8% in the least deprived decile (Child and Maternal Health, 2024). Geographical variations data are also not available for this indicator. Geographical variations data are also not available for this indicator.
Population vaccination coverage: PCV booster
The PCV vaccine protects against pneumococcal infections that can cause pneumonia, septicaemia or meningitis. The PCV vaccine is given to all children under two years old as part of the childhood vaccination programme. This indicator is defined as ‘Children for whom the local authority is responsible who received a booster dose of PCV vaccine at any time by their second birthday as a percentage of all children whose second birthday falls within the time period.’
PCV booster coverage in Bury for the period 2023/24 was at 84.1%, lower than the North West average of 87.8% and statistically worse than England average of 88.2%. The coverage in all three areas is below the national target of 95% and Bury needs to vaccinate 249 additional children to reach the national target.
Examining trend data from 2010 to 2024, vaccination coverage for the PCV booster in Bury steadily increased from 89.3% in 2010/11 to the highest coverage at 93.9% in 2013/14. This was followed by a decline from 93.4% in 2014/15 to 87.9% in 2018/19. Coverage then increased from 89% in 2019/20 to 90.2% in 2021/22, followed by two periods of decrease to 88% in 2022/23 and then to its lowest level of 84.1% in 2023/24. Based on the 5 most recent data points, coverage in Bury is decreasing (statistically significant) and getting worse.
England saw an increase in vaccination coverage from 89.3% in 2010/11 to the highest at 92.5% in 2012/13. Coverage remained stable until 2014/15 at 92.2%, before seeing a gradual decline to 88.2% in 2023/24 (Figure 13).
Figure 13: PCV booster coverage for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Bury has the lowest PCV booster coverage in its group of six statistical children service neighbours, with the highest percentage in Stockton-on-Tees at 93% for the year 2023/24 (Children and Maternal Health, 2024). There are no data on inequalities at Bury level but England data suggests decreasing coverage of PCV booster with increasing levels of deprivation. The most deprived decile in England has a coverage of 83% compared with 91.6% in the second least deprived decile and 90.6% in the least deprived decile for the year 2023/24 (Child and Maternal Health, 2024).
No geographical data are present for the MMR vaccine by PCN. GP level data are available here.
Emergency care
In England, both Accident & Emergency (A&E) visits and subsequent emergency admissions for infants have increased significantly over the past 15 years. Hospital contact rates among children peak during infancy (one year old), with infants also having the highest proportion of 'inappropriate' accident and emergency (A&E) attendances (attendances to an emergency department that did not result in an admission or any treatment/intervention). Bronchiolitis, upper respiratory viral infections, intestinal infections, gastroenteritis, jaundice, and feeding difficulties are the most common reasons for infant admissions to A&E departments (Nath et al, 2022). Unintentional injuries form a major burden of disease in children and young people and are a major cause of inequality. Unintentional injuries in and around the home are a leading cause of preventable death for children under five years and are a major cause of ill health and serious disability.
A&E attendance 0-4 years old
A&E attendances in children aged under five years are often preventable, and commonly caused by accidental injury or by minor illnesses which could have been treated in primary care. Bury has a crude A&E attendance of 704.1 in the period 2023/24, lower (statistically significant) than the England average of 750.7 per 1,000 (Maternal and Child Health, 2024). The figure for Bury has decreased since 2021/22 from 790.2, going from significantly worse than England to its current rate in 2023/24 of 704.1 per 1,000 and significantly better than England average. The rate for England has increased over the same time period, increasing from 762.6 per 1,000 to 750.7 per 1,000 population aged 0-4 years (Figure 14).
Figure 14: Crude A&E attendance per 1,000 population aged 0-4 years for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Amongst Bury’s group of statistical neighbours, Bury has the eighth highest A&E attendance per 1,000 population aged 0-4 years for 2023/24, with the highest rate in Stockton-on-Tees at 1,198.2 per 1,000 and lowest in Bracknell Forest at 534.4 per 1,000 (Maternal and Child Health, 2024).
Data on inequalities are present by sex and age for Bury. Data by sex suggest higher A&E attendance rates of 753.1 per 1,000 in males (statistically higher than Bury average) compared with 650.9 per 1,000 in females for 2022/23 (statistically lower than Bury average) (Maternal and Child Health, 2024). Data by age group suggests higher admission rates in children under 1 years of age (1,129 per 1,000) compared with the 1-4 years (607 per 1000) age group.
Data on inequalities at England level are available by sex, deprivation and age for the year 2023/24 . Similar to Bury, males have a higher rate of A&E admissions at 810.1 per 1,000 compared with females at 688.4 per 1,000 for 2023/24. Examining data by levels of deprivation, the highest A&E attendance rate are in the two most deprived deciles (882.3 in decile 1 and 906.4 in decile 2), decreasing with lower levels of deprivation to 605 per 1,000 in the least deprived decile. Data by age group suggests higher admission rates in children under 1 years of age (1,174.9 per 1,000) compared with the 1-4 years (653.1 per 1000) age group.
Emergency admissions (aged 0-4)
Emergency admissions account for approximately 35% of all NHS admissions in England, costing roughly £11 billion per year. Admitting a patient to the hospital as an emergency is expensive and frequently avoidable, yet the number of emergency admissions to hospitals has been increasing for some time. In terms of public health, emergency admissions data provide an indication of broader determinants of poor health, such as housing and transportation. In 2014/15, respiratory infections accounted for more than one-quarter of all emergency hospital admissions in children under the age of five. Smoking in the home and damp housing have been linked to an increase in the risk and severity of respiratory infections in young children (Maternal and Child Health, 2024).
Emergency admissions for children aged 0-4 years are available as crude rate per 1,000 population aged 0-4 years. In 2023/24, Bury had an emergency admission rate of 96 for children aged 0-4 years per 1,000 population, lower (statistically significant) than the England average of 151 per 1,000 (Maternal and Child Health, 2024).
Trend data based on 5 most recent data points suggests that the emergency admissions rates for children aged 0-4 years rates in Bury are decreasing and getting better (statistically significant). The rates in Bury gradually increased from 220 per 1,000 population aged 0-4 years in 2010/11 to 246 per 1,000 in 2012/13. This was followed by a decline until 2014/15 with a rate of 198 per 1,000 population aged 0-4 years. However, rates then increased from 206 in 2015/16 to 285 per 1,000 population in 2018/19, before decreasing slightly in 2019/20 to 253. The year 2020/21 saw a sharp decline in emergency admissions rates for children aged 0-4 years to 133 per 1,000. This was followed by a significant increase to 207 per 1,000 in 2021/22, then two further periods of decrease to 164 in 2022/23 and then to 96 per 1,000 in 2023/24, Bury’s lowest rate to date. Throughout the period 2010/11 to 2021/22, the rates in Bury remained significantly worse than England average. However in 2022/23, Bury was statistically similar to England, and then for the most recent time period 2023/24, Bury is now statistically better than England average.
In England as a whole, there was a decline in emergency admission rates from 150 in 2010/11 to 148 in 2014/15. This was followed by an increase over the years to 172 in 2018/19, before declining to 167 in 2019/20. Similar to Bury, England saw a sharp decline with emergency admission rates at 94 in 2020/21, followed by a sharp increase in 2021/22 to 161 per 1,000. The rate has since gradually decreased in England to 158 for 2022/23 and then to 151 for 2023/24 (Figure 15).
The sharp decline observed in Bury and England can be explained by the COVID-19 pandemic, that had a large impact on hospital activity with a reduction in admissions in 2020 to 2021.
Figure 15: Emergency admission rates per 1,000 population aged 0-4 years for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Bury has the lowest rate of emergency admissions in its group of 6 statistical children service neighbours, with the highest rate in Stockton-on-Tees at 247 per 1,000 for the year 2023/24 (Children and Maternal Health, 2024).
Data on inequalities for Bury are available by sex only with higher rates in males (102 per 1,000) compared with females (89 per 1,000) (Child and Maternal Health, 2024). England data are available by sex and levels of deprivation. Similar to Bury, males have a higher admission rate (167 per 1,000) compared with females (134 per 1,000) for 2023/24. Data by deprivation based on LSOA deprivation deciles suggests increasing emergency admission rates with increasing levels of deprivation. The most deprived decile in England has an admission rate of 187, compared with 45 in the least deprived decile for the year 2022/23 (Child and Maternal Health, 2023).
Geographical variations in Emergency admissions (aged 0-4)
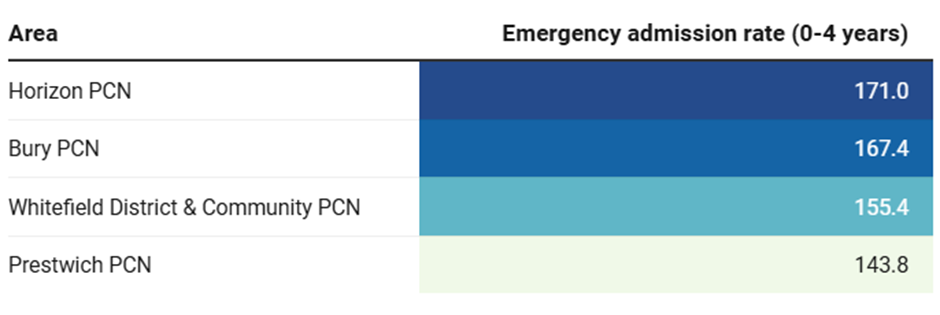
Data on geographical inequalities are available at both PCN and GP levels. We will be presenting data at PCN levels only. Data at GP levels are available here.
Crude emergency admission rates per 1,000 population aged 0-4 years for the period 2020/21 to 2022/23 is highest in Horizon PCN at 171 and lowest in Prestwich PCN at 143.8 (Table 8).
Table 8: Emergency admission rates per 1,000 population aged 0-4 years across primary care networks in Bury, 2020/21-22/23 (National General Practices Profile, 2023)
Injuries
Injuries are a leading cause of hospitalisation and premature mortality in children and adolescents. They are also a source of long-term health problems, such as mental health issues related to the experience(s). Unintentional injuries in and around the home are a leading cause of preventable death for children under five years and are a major cause of ill health and serious disability.
Hospital admissions caused by unintentional and deliberate injuries in children (aged 0 to 4 years)
The admissions data are available as crude rate of hospital admissions caused by unintentional and deliberate injuries in children aged under 5 years per 10,000 resident population aged under 5 years.
Hospital admissions caused by unintentional and deliberate injuries in children (aged 0 to 4 years) in the period 2023/24 for Bury are 81.8 per 10,000 resident population aged under 5 years, statistically similar to the England average of 93.2. (Maternal and Child Health, 2024). The rate of hospital admissions caused by unintentional and deliberate injuries in children aged 0 to 4 has decreased over time in Bury, from 214.3 per 10,000 in 2010/11 to 81.8 in 2023/24. The rate has fluctuated over the years, reaching its peak in 2013/14 at 239.3 per 10,000. The rate has steadily declined from 2018/19 to reach its lowest level of 81.8 in 2023/24. Bury has remained significantly worse than England from 2010/11 to 2021/22, then for the latest two time periods 2022/23 and 2023/24 Bury has been statistically similar to England in this measure (Figure 16). Trend data based on 5 most recent data points suggests that the hospital admission rates for children aged 0-4 years rates in Bury are decreasing and getting better (statistically significant). The rate in England has also decreased from 143.4 in 2010/11 to 93.2 in 2023/24. The rate in England has remained relatively stable, showing a gradual decrease from its peak in 2011/12 at 148.3 per 10,000 to its lowest rate in 2022/23 of 92 per 10,000, followed by a slight increase in the latest time period to 93.2 for 2023/24.
Figure 16: Hospital admissions caused by unintentional and deliberate injuries in children (aged 0 to 4 years) (Crude rate – per 10,000) for Bury and England from the year 2010/11 to 2023/24 (Child and Maternal Health, 2024)

Amongst Bury’s group of six statistical children service neighbours, Bury has the lowest hospital admissions, with the highest rate in Calderdale at 147 per 10,000 for 2023/24 (Maternal and Child Health, 2024).
Data on inequalities are present by sex only for Bury, that suggests higher hospital admissions rates in males of 96.1 per 10,000 resident population aged under 5 years (statistically similar to Bury average) compared with 66.3 per 10,000 in females for 2023/24 (statistically similar to Bury average) (Maternal and Child Health, 2024).
Data on inequalities at England level are available by sex and deprivation. Similar to Bury, males have a higher rate of hospital admissions at 103.2 per 10,000 compared with females at 82 per 10,000 resident population aged under 5 years for 2023/24. Examining data by levels of deprivation, the highest hospital admissions rate is in the most deprived decile (109.3 in decile 1) and the lowest in the third least deprived decile (79.9 per 10,000 resident population aged under 5 years) and the least deprived decile (85.9 per 10,000 resident population aged under 5 years) (Maternal and Child Health, 2024).
Children aged 5 and under killed or seriously injured in road traffic accidents (RTA)
Road traffic accidents are a leading cause of death in children, accounting for a greater proportion of accidental deaths as children grow older. Parents cite vehicle speed and volume as reasons for not allowing their children to walk or cycle, limiting physical activity opportunities (Maternal and Child Health, 2024).
This indicator is measured as a crude rate of children aged 0-5 years who were killed or seriously injured in road traffic accidents per 100,000 population.
The rate of road traffic accidents that have killed or seriously injured children under 5 years of age in Bury was 2.5 per 100,000 for the period 2020-22, with one child having been killed in this time period. The rate in the North West for the same time period is 10 per 100,000 population, which higher (statistically significant) than the England average of 7.5 (Maternal and Child Health, 2024).
Amongst Bury’s group of 6 statistical children service neighbours, Bury has the second lowest rate of road traffic accidents that have killed or seriously injured children under 5 years of age for 2020-22. Lancashire has the highest rate of children aged 0-5 years who were killed or seriously injured in road traffic accidents at 14.5, and Stockport had the lowest rate (1.7 per 100,000) (Maternal and Child Health, 2024).
Early Childhood Development
There are limited data on child development at 2-2 ½ years of age for Bury with data for some years missing. Where data are available, there are concerns about the quality of the data. However, data are available on development at the end of the Early Years Foundation Stage (EYFS) measured as school readiness.
School readiness is a key measure of early years development across a wide range of developmental areas. Children from more deprived backgrounds are at a greater risk of poorer development and the evidence shows that differences by social background emerge early in life.
School readiness: percentage of children achieving a good level of development at the end of Reception
This measure is defined as ‘Children defined as having reached a good level of development at the end of the Early Years Foundation Stage (EYFS) as a percentage of all eligible children’.
Examining the data for Bury for the year 2023/24, 65% of children achieved a good level of development at the end of Reception, lower (statistically significant) than the England average of 67.7% but slightly higher than the North West average of 64.4% (Maternal and Child Health, 2024). The percentage of children that achieved a good level of development at the end of Reception has increased in Bury from 63.3% in 2021/22 to 65.7% in 2022/23, both of which were statistically similar to the England average. However, the latest decline has left Bury worse (statistically worse) than England, with the proportion in England increasing from 65.2% in 2021/22 to 67.7% in 2023/24 (Figure 17).
Figure 17: School readiness: percentage of children achieving a good level of development at the end of Reception (%) for Bury and England from 2021/22 to 2023/24 (Child and Maternal Health, 2024)

Amongst Bury’s group of statistical neighbours, Bury ranks 4th in its group of 6 children’s services statistical neighbours with the highest percentage of children achieving a good level of development at the end of Reception in Stockton-on-Tees at 69.5% and lowest in Sefton at 62.7% (Maternal and Child Health, 2024).
Data on inequalities at Bury level are only available by sex and by free school meals status. Data from 2023/24 shows that a lower percentage of males (58%, significantly lower than Bury average) in Bury achieve a good level of development at the end of Reception compared with females (73.5%, significantly higher than Bury average) (Maternal and Child Health, 2024). Only 48.7% with a record of free meal status achieve a good level of development at the end of Reception, similar to England average of 51.5% for 2023/24 (Maternal and Child Health, 2024).
Data on inequalities at England level are available by sex, deprivation, month born, special education needs (SEN) status, first language status and ethnic group for the year 2023/24.
Similar to Bury, a lower percentage (60.7%) of males in England achieve a good level of development at the end of Reception compared with females (75%) for 2023/24. Data by deprivation for England shows that as the levels of deprivation increases, the percentage of children who reach a good level of development at the end of reception decreases. 62.8% of children in the most deprived decile (decile 1) reached a good level of development compared with 71.7% in the least deprived decile (decile 10) for 2023/24. Examining data by ethnic groups, a higher proportion of children from mixed/multiple ethnic groups (69.5%) reached a good level of development at the end of Reception, followed by white ethnic group (69.2%) and Asian/Asian British including Chinese (66.9%). Black/African/Caribbean/Black British (62.3%) and other ethnic groups (60.2%) have the lowest proportion of children reaching a good level of development for 2023/24. Comparing school readiness by SEN, a higher proportion of children with no identified SEN (75.6%) achieve a good level of development at the end of Reception compared with development in those children receiving SEN support (24.9%) and with a statement or EHCP (3.8%) for 2023/24.
No data on geographical variations in Bury are available.
School readiness: percentage of children achieving at least the expected level in communication and language skills at the end of Reception
According to the 2018-2019 remit letter, the Office for Health Improvement and Disparities is expected to drive improvements in outcomes at scale, with a particular focus on child health speech, language, and communication needs, and school readiness. Disparities in child language abilities are noticeable in the second year of life and have a clear impact by the time children enter school. If these children are not supported, they are more likely to fall short of their full potential. The Office for Health Improvement and Disparities has received funding to train Health Visitors in the use of a new communication and language assessment tool to identify problems at 2 to 2 and a half years of age and to plan interventions for children who are developing below the expected level.
As part of the Department for Education's (DfE) plan to improve social mobility through education, their ambition to close the "word gap" focuses on the development of key early language and literacy skills for disadvantaged pupils or those not achieving their full potential.
Each year, the Early Years Foundation Stage Profile is used to inform child development plans, informing Key Stage 1 teachers and parents about each child's development and needs. The data from the communication and language early learning goal check provides teachers and service planners with information on children's ability to communicate effectively and whether additional intervention is required to meet the standard.
The communication and language development indicator of school readiness is used to measure the impact of Early Years services (including the universal and non-universal aspects of health visiting) and also regarded as an important social determinant of longer-term health, education and life chances. It is defined as ‘Children defined as having reached at least the expected level of development in communication and language skills at the end of the Early Years Foundation Stage (EYFS) as a percentage of all eligible children.’ (Maternal and Child Health, 2024).
Examining the data for Bury for the year 2023/24, 78.1% of children achieved at least the expected level in communication and language skills at the end of Reception, statistically similar to the England average of 79.3% (Maternal and Child Health, 2024). There has been a slight decline from 80% in 2021/22 to 78.1% in 2023/24, consistent with the slight reduction seen in England from 79.5% to 79.3% for the same time period (Figure 18). The rate in Bury has remained statistically similar to England for the observed time period.
Figure 18: School readiness: percentage of children achieving at least the expected level in communication and language skills at the end of Reception (%) for Bury and England from 2021/22 to 2023/24 (Child and Maternal Health, 2024)

Among Bury’s group of six statistical neighbours for children’s services, Bury ranks fourth for the expected level of communication and language skills in 2023/24. Stockport recorded the highest percentage at 80.6%, while Sefton had the lowest at 75.9% (Maternal and Child Health, 2024).
Data on inequalities at Bury level are only available by sex. In the year 2023/24, higher percentage (84.6%) of females achieve at least the expected level in communication and language skills (statistically better than Bury average) when compared to males at 72.8% (statistically worse than Bury average), consistent with the percentages in England (85.3% for females and 73.7% for males). Data on inequalities at England level are also available by deprivation, free school meal status, month born, special education needs (SEN) status, first language status and ethnic group for the year 2023/24.
Only 68.2% of children with a free school meal status achieved the communication and language skills compared with 82.4% of children not eligible for free school meals for 2023/24. Data by deprivation for England shows that as the levels of deprivation increases, the percentage of children who achieve at least the expected level in communication and language skills at the end of reception decreases. Around 74.2% of children in the most deprived decile (decile 1) achieve at least the expected level compared with 83.3% in the least deprived decile (decile 10) for 2023/24. Examining data by ethnic groups, a higher proportion of children from white ethnic groups (81.8%) achieve at least the expected level in communication and language skills, followed by mixed/multiple ethnic groups (80.5%) and Asian/Asian British including Chinese (74.9%). Black/African/Caribbean/Black British (72.2%) and other ethnic groups (69.9%) have the lowest proportion of children achieving at least the expected level for 2023/24. Comparing school readiness by SEN, a higher proportion of children with no identified SEN (87.3%) achieve at least the expected level in communication and language skills compared with children receiving SEN support (38.2%) and with a statement or EHCP (7.6%) for 2023/24.
There are no data on geographical variations in Bury.
Oral Health
The most common dental pathologies in the UK are dental caries (tooth decay) and periodontal (gum) disease. Tooth decay has become less common in the last two decades, but it remains a major health and social issue. It causes tooth crown destruction and frequently causes pain and infection. Dental disease is more prevalent in deprived areas than in affluent communities.
Hospital admissions for dental caries (0-5 years) is a good direct measure of dental health as well as an indirect, proxy measure of child health and diet (Maternal and Child Health, 2024). It is defined as ‘Finished consultant episodes for dental caries among children aged 0-5, rate per 100,000 population aged 0-5 years’
Examining the data for Bury for the period 2021/22 to 2023/24, the admission rate in Bury was higher (statistically significant) at 261.3 per 100,000 than the England average of 207.2 per 100,000.
Between the periods 2015/16–2017/18 and 2017/18–2019/20, hospital admissions for dental caries among children in Bury declined from 448.0 to 404.6 per 100,000 population. A similar downward trend was observed nationally, with the rate in England decreasing from 331.2 to 294.5 per 100,000.
A more pronounced decline occurred during 2018/19–2020/21, with Bury’s rate falling to 235.9 per 100,000, and England’s to 227.9 per 100,000. This sharp reduction is likely attributable to the impact of the COVID-19 pandemic on hospital service utilisation, rather than a genuine improvement in oral health or dietary behaviours among children. The downward trend continued into 2019/20–2021/22, with rates further reducing to 192.6 in Bury and 197.5 in England. However, this was followed by a reversal in Bury, where the rate increased to 233.1 per 100,000 in 2020/21–2022/23, and further to 261.3 per 100,000 in 2021/22–2023/24. In contrast, England experienced a continued decline to 178.8 per 100,000 in 2020/21–2022/23, before a slight increase to 207.2 per 100,000 in 2021/22–2023/24 (Figure 19).
Figure 19: Hospital admissions for dental caries (0-5 years) per 100,000 population aged 0-4 years for Bury and England from the year 2015/16 – 2017/18 to 2021/22 – 2023/24 (Child and Maternal Health, 2024)

Bury has the 7th highest hospital admission rates for dental caries (0-5 years) in its group of 16 similar local authorities, with the lowest rate in Warrington at 77.6 per 100,000 and highest in Telford and Wrekin at 400.5 for the period 2021/22-2023/24 (Children and Maternal Health, 2024).
Data on inequalities for Bury are available by sex only for the period 2021/22-2023/24 with higher rates in males (313.9 per 100,000) compared with females (205.4 per 100,000) (Child and Maternal Health, 2024). However, the difference by sex in Bury are not statistically significant. England data are available by sex and levels of deprivation for the same time period. Males aged 0-4 years have higher (statistically significant) admission rates for dental caries (223.6.6 per 100,000) compared with females (186.8 per 100,000). Data by deprivation (based on LSOA deprivation deciles) suggests increasing hospital admission rates for dental caries (0-5 years) with increasing levels of deprivation. The most deprived decile in England has an admission rate of 265.8 compared with 87.9 in the least deprived decile for the period 2018/19-2020/21 (Child and Maternal Health, 2024).