Pregnancy and Birth
Pregnancy and Birth
Pregnancy and Birth
The foundation of a child’s future health and development is laid in the womb, making pregnancy an important period. Maternal exposure and experiences during this critical period can have long-term impact of the physical and mental health and wellbeing of a child throughout their life course.
In addition to influencing child development by affecting foetal development, maternal health and behavioural risk factors can influence the risk of adverse health outcomes later in life including cardiovascular diseases, diabetes, and mental health disorders. These risk factors include poor maternal nutrition, smoking during pregnancy, alcohol use and exposure to environmental toxins. On the other hand, good prenatal care, a healthy diet, and other positive behaviours can help promote foetal growth and development and reduce the risk of adverse health outcomes in the child.
It is important to note that the effects of pregnancy on a child's development and life course are not solely determined by the maternal behaviour and experiences. Wider determinants of health including social, economic, and environmental context in which the mother and child live can also have a significant impact on the child's health and development. For example, poverty, lack of access to healthcare, and exposure to violence and air pollution can all increase the risk of adverse health outcomes for both the mother and child. Understanding patterns in health before and during pregnancy is important if we are to narrow the health gap for those who are most vulnerable. Inequalities in maternal and infant outcomes exist, with poorer outcomes experienced by certain groups of women and their babies.
Maternal Health Outcomes
Maternal health is the health of women during pregnancy, childbirth and the post-partum period. It encompasses the healthcare dimension of preconception, prenatal and postnatal care, to ensure a positive and fulfilling experience, and reduce maternal morbidity and mortality. Each stage should be a positive experience, ensuring women and their babies reach their full potential for health and well-being (WHO, 2023).
Monitoring maternal health outcomes allows us to identify areas where improvements are needed and implement interventions to reduce maternal morbidity and mortality. They also allow us to monitor progress towards achieving global health targets, such as the Sustainable Development Goals (SDGs 3 and 5) and the World Health Organization's (WHO) Global Strategy for Women's, Children's and Adolescents' Health. These targets include reducing maternal mortality, improving access to maternal health services, and promoting maternal and new-born health.
In this section, we will provide an overview of reproductive health using the general fertility rate indicator, followed by indicators on health behaviours and risk factors in pregnancy, maternal health screening and health care access. The data are sourced from the child and maternal health profile and where comparisons are made, they include the 'closest 4' children's services statistical neighbours and England.
a. General Fertility Rate:
General fertility rate (GFR) is an important measure of reproductive health and provides useful insights into the demographic composition and health status of a population. It is the number of live births each year per 1,000 women aged 15 to 44 years. GFR is a more refined measure of fertility than the crude birth rate as it considers the age distribution of women in their reproductive years.
Data on general fertility rates prior to 2016 for Bury are not available. General fertility rates in Bury have remained stable between 2017 to 2019 with 64.7 live births per 1000 women aged 15-44 years in 2017 to 63.8 per 1000 women aged 15-44 years in 2018 and 2019. This was followed by a decline during the COVID-19 pandemic to 60.6 in 2020 and 58.1 in 2021. In England, there was continuous decline in GFR from 61.2 live births per 1000 women aged 15-44 years in 2017 to 54.3 in 2021. (Figure 3).
Figure 1: Comparison of GFR by usual area of residence for the years 2017 to 2021 for Bury and England
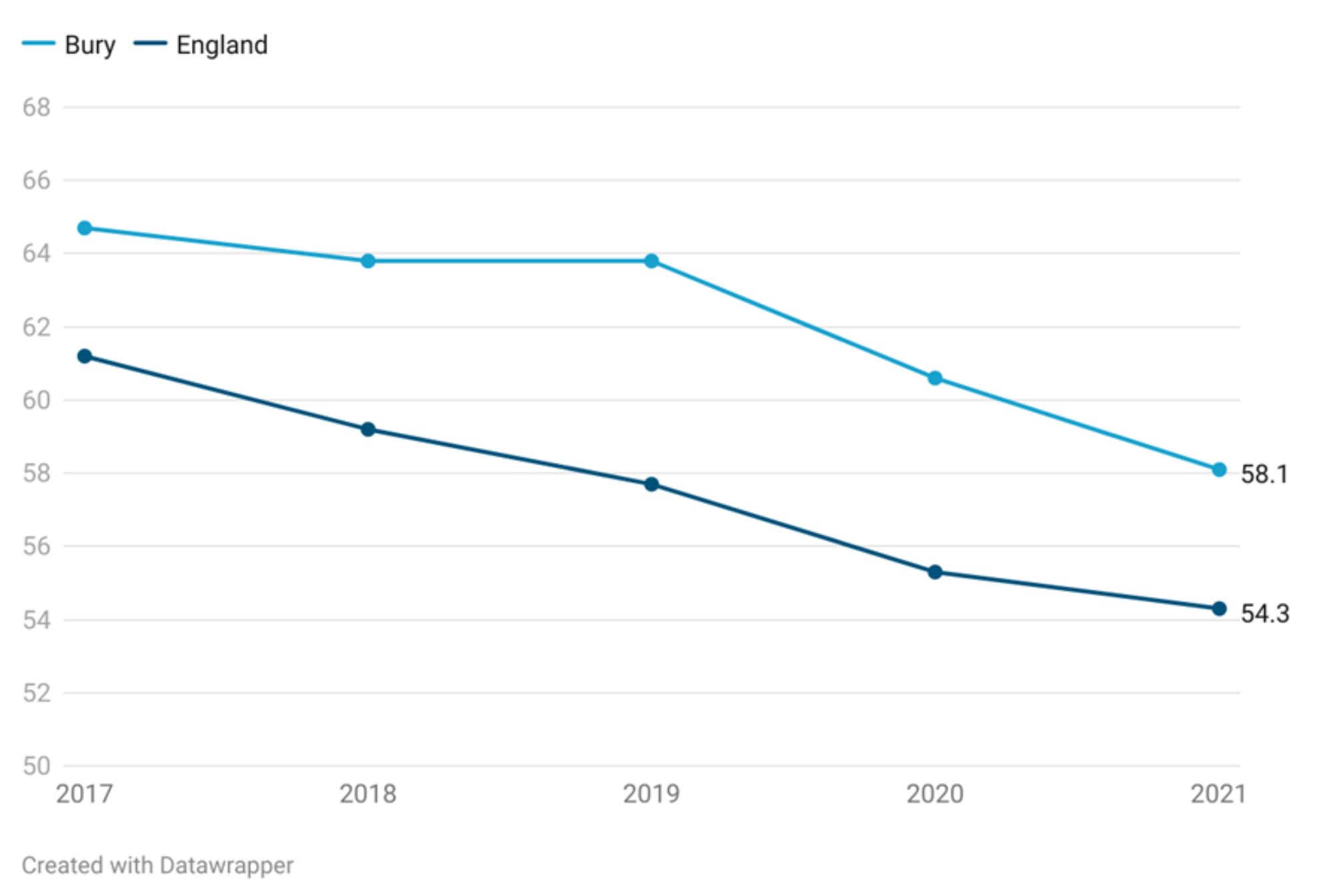
The General fertility rate in Bury has remained above England average over the period 2017-2021. This may be due to several factors:
Demographic factors: The age distribution and ethnic composition of a local population can influence the GFR. For example, if a local authority has a higher proportion of women of childbearing age, this can increase the number of live births and raise the GFR. This does not appear to be the case for Bury, where 18% of the population is of childbearing age compared with 19.5% in England.
Socioeconomic factors: Education levels, employment status, and income can also play a role in determining the GFR. Higher levels of education and income are often associated with lower fertility rates, while areas with higher levels of unemployment and poverty may have higher fertility rates.
Cultural factors: Attitudes towards family size and childbearing can vary between regions and communities. For example, some cultural or religious groups may place a strong emphasis on having large families, which can raise the GFR in those areas.
Healthcare access: Access to family planning services and healthcare can also impact the GFR. Areas with better access to reproductive health services and education are likely to have lower GFRs compared to areas with limited access.
It is important to note that the GFR can fluctuate over time and may be influenced by short-term events or changes in policy or initiatives. A higher GFR compared to the national level does not necessarily indicate a better or worse standard of living.
b. Preconception
Preconception health is a woman's health before she becomes pregnant. It focuses on factors to protect the health of a baby they might have some time in the future. This section examines indicators relevant to preconception.
Many of the available indicators relate to birth control. This is because physical and mental health outcomes for both the child and mother are better on average when a pregnancy is intentional.
Long-acting reversible contraceptive
Long-acting reversible contraceptive (LARC) methods, such as contraceptive injections, implants, the intra-uterine system (IUS) or the intrauterine device (IUD), are highly effective as they do not rely on daily compliance and are more cost effective than condoms and the pill. A strategic priority is to ensure access to the full range of contraception is available to all. An increase in the provision of LARC is a proxy measure for wider access to the range of possible contraceptive methods and should also lead to a reduction in rates of unintended pregnancy. Fingertips measures the provision of LARC but excludes injections with one of the key reason being that injections are primarily outside local authority contracts. [SS1]
Long-acting reversible contraceptive under 25s
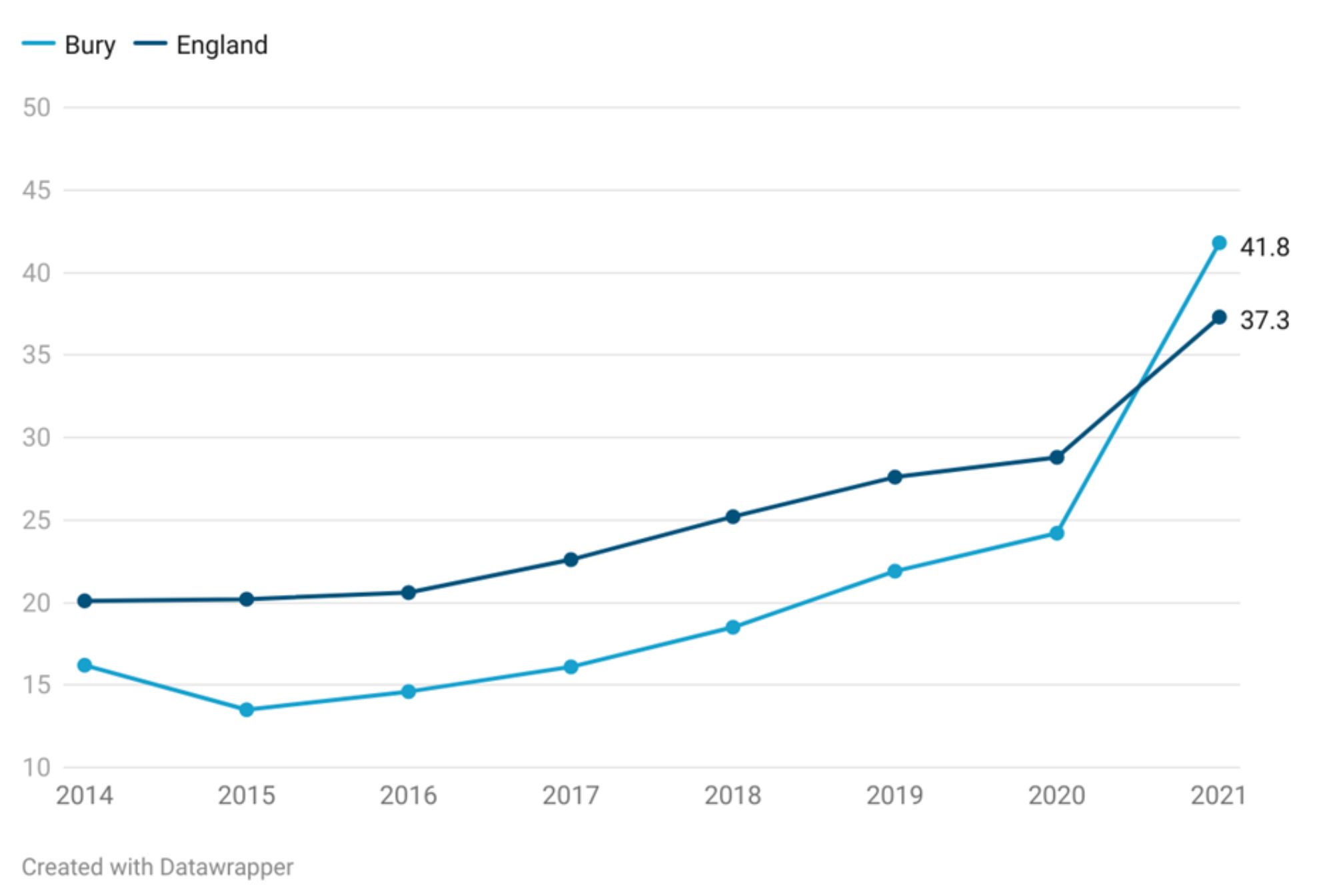
In the year 2021, approximately 41.8% of under 25s chose LARC excluding injections at SRH Services (%) higher (statistically significant) than 37.3% in England. Bury has seen an increase in under 25s who choose LARC from 16.2% in 2014 to 41.8% in 2021. An increase has been seen in England but at a slower rate with under 25s who choose LARC increasing from 20.1% in 2014 to 37.3% in 2021.
This bit needs a bit more explaining in how it's relevant to baby's health. I'd suggest putting it first under pre-conception with some words about how preveting unwanted pregnancies protects mum's physical and mental health and babies get the best start if they are the result of planned conceptions. [SS1]
Figure 4: Comparison of percentage (%) of Under 25s choosing LARC excluding injections at SRH Services for the years 2014 to 2021 for Bury and England
Bury has the 5th highest percentage (%) of Under 25s choosing LARC excluding injections at SRH Services in its group of similar local authorities in 2021 with the lowest percentage in Doncaster at 13.4% and highest in Rotherham at 58.2% (Sexual & reproductive health profiles, 2021). There are no data on inequalities at Bury level and England data does not show any deprivation gradient.
Long-acting reversible contraceptive over 25s
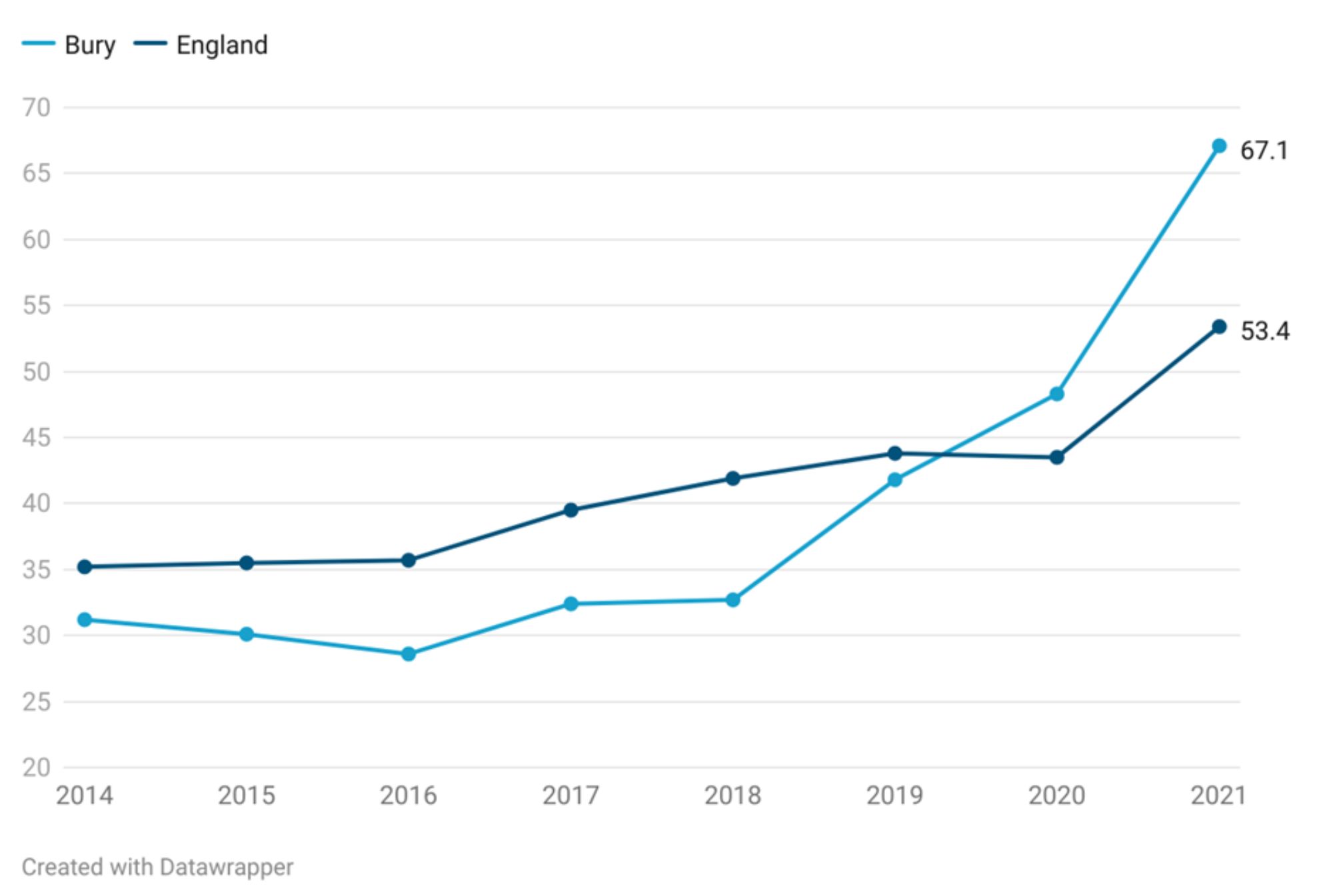
In the year 2021, approximately 63.3% of over 25s chose LARC excluding injections at SRH Services (%) higher (statistically significant) than 53.4% in England. Bury has seen a steady increase in over 25s who choose LARC from 31.2% in 2014 to 32.7% in 2018. This was followed by a sharp rise to 41.8% in 2019, 48.3% in 2020. England saw a slower rate of increase with over 25s who choose LARC increasing from 35.2% in 2014 to 43.5% in 2020. Both Bury and England saw a sharp rise in the percentage of over 25s choosing LARC in 2021 where the percentage increased to 63.3% in Bury (18.4% increase from 2020) and 53.4% (9.9% increase from 2020) in England.
Figure 5: Comparison of percentage (%) of over 25s choosing LARC excluding injections at SRH Services for the years 2014 to 2021 for Bury and England
Bury has the 4h highest percentage (%) of over 25s choosing LARC excluding injections at SRH Services in its group of similar local authorities in 2021 with the highest percentage in Rotherham at 78.5% and lowest in Doncaster at 30.9% (Sexual & reproductive health profiles, 2021). There are no data on inequalities at Bury level and England data does not show any deprivation gradient.
Under 18 conception rates
Maternal age is an important factor for pregnancy outcomes. Younger women are at higher risk of adverse pregnancy outcomes. For example, they are less likely to take a folic acid supplement which protects against the risk of neural tube defects such as spina bifida (Bestwick et al, 2014). Babies born to women under the age of 20 are also approximately 20% more likely to be of low birth weight (ONS, 2023). Teenage mothers are less likely to complete their education, are more likely to raise their child alone and in poverty, and are at a greater risk for mental illness than their older counterparts. The infant mortality rate for babies born to teenage mothers is approximately 60% higher than that of babies born to older mothers. The children of teenage mothers are more likely to live in poverty and substandard housing, and to experience accidents and behavioural issues. Raising a child as a teenager is difficult and frequently results in negative outcomes for the baby's health, the mother's emotional health and well-being, and the likelihood of both parent and child living in long-term poverty (OHID, 2023).
During the period 2021-22, 0.5% of the pregnancies were teenage pregnancies (Percentage of delivery episodes, where the mother is aged under 18 years) statistically similar to 0.6% in England. The percentage of pregnancies in under 18s has been declining both nationally and in Bury (Children and Maternal Health, 2021)
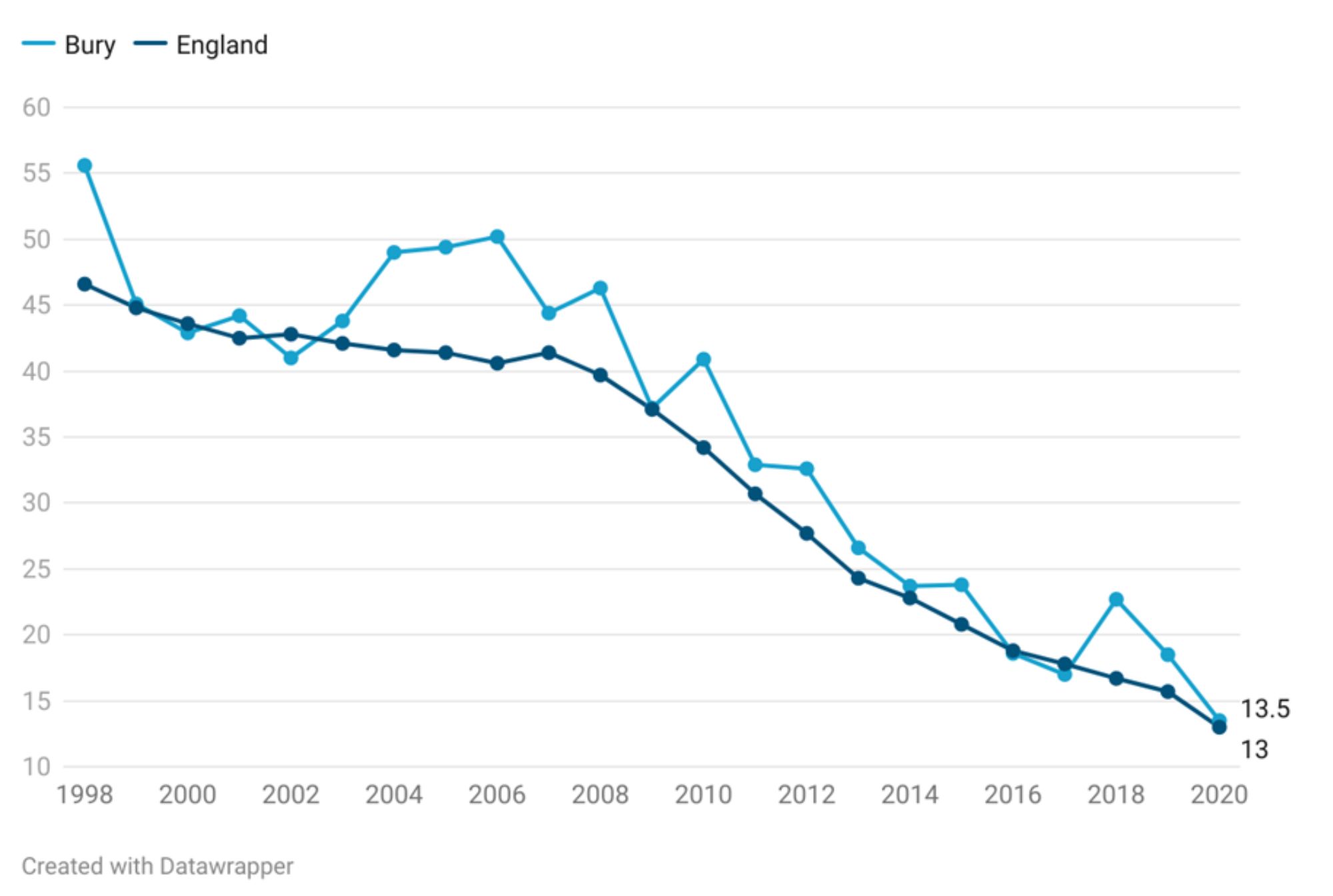
Under 18 conception rate is measured as conceptions in women aged under 18 per 1,000 females aged 15-17 years. The rate for Bury in the year 2020 was 13.5 per 1000 females aged 15-17 years statistically similar to England average of 13. There has been a downwards trend in the under 18 conception rates for Bury and England from 1998 to 2020 (Figure 2), however the rates in Bury have remained consistently higher than England during this period. The rate in Bury declined from the peak at 55.6 per 1000 females in 1998 and gradually declined to 13.5 per 1000 females in 2020. In 1998, the under 18 conception rate in England was 46.6 per 1000 females, and it gradually declined to 13 per 1000 females in 2020. A recent study has attributed this decline to local areas experiencing less youth unemployment, growing Black or South Asian teenage populations, more educational attainment, unaffordable housing, and a lack of available social housing (Heap et al, 2020).
Figure 3: Comparison of conceptions in women aged under 18 per 1,000 females aged 15-17 years for the years 1998 to 2020 for Bury and England
Compared to Bury closest children's services statistical neighbours, Bury has the second lowest under-18 conception rate in its group of 5 statistical children service neighbours with the highest rate in Stockton-on-tees at 22 and lowest in Stockport at 13.1 (Children and Maternal Health, 2020). There are no data on inequalities at Bury level but England data suggests increasing conception rates with increasing levels of deprivation. The most deprived decile in England has an under-18 conception rate of 18.6 compared with 7.5 in the least deprived decile for the year 2020 (Child and Maternal Health, 2020).
Under 18 conceptions leading to abortion
It is increasingly common for pregnant young women under 18 to have an abortion. Access to family planning and sexual health services, and the availability of independent sector abortion provision, directly affect abortion proportions. More deprived areas in England have both higher conception rates and a lower proportion of under-18 pregnancies ending in abortion.
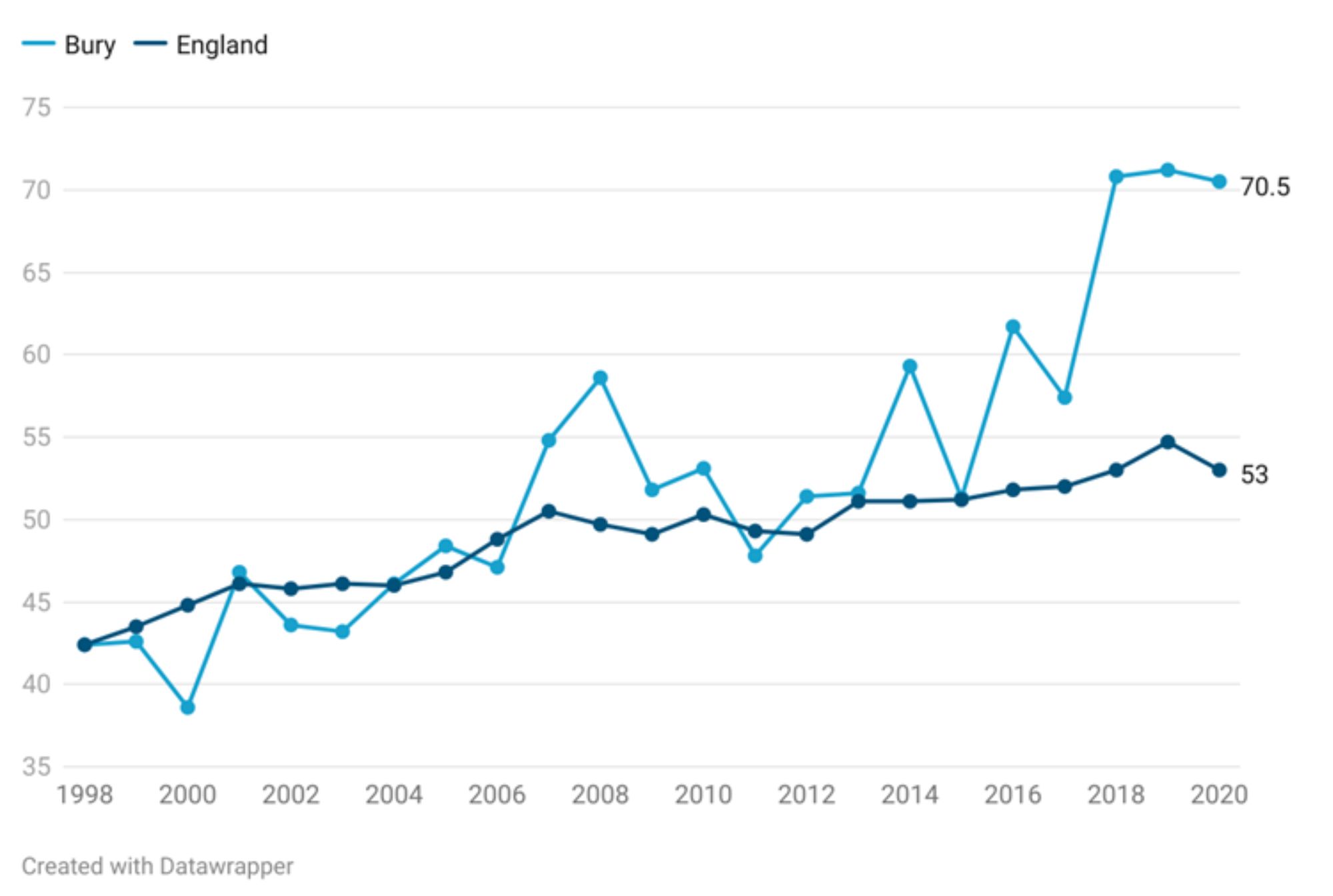
Most recent data for Bury shows that 70.5% of under 18 conceptions led to abortion, higher (statistically significant) than England average of 53%. Figure 4 presents the percentage of conceptions to those aged under 18 years that led to an abortion in Bury and England from the year 1998 to 2020. The percentage of abortions in Bury ranged from 38.6% in 2000 to 71.2% in 2019. From the year 1998 to 2000, there was a decrease in the percentage of abortions from 42.4% to 38.6% and then started to increase again. From the year 2001, the percentage of under 18 conceptions leading to abortion continued to increase from 46.8% to reach a peak of 71.2% in 2019, before decreasing slightly to 70.5% in 2020. The large fluctuation in data for Bury may be due to small numbers at the local level.
The trend in England is different from that observed in Bury with less fluctuation in the data ranging from 42.4% to 53% from 1998 to 2020. The percentage of abortions in under-18s increased steadily from 42.4% in 1998 to 50.5% in 2007, remaining stable until 2012 at 49.1% before steadily increasing to the peak in 2019 at 54.7% and slightly declining to 53% in 2020 (Figure 4).
Figure 4: Comparison of percentage (%) of under 18 conceptions leading to abortions for the years 1998 to 2020 for Bury and England
Bury has the highest under 18 conceptions leading to abortion in its group of 5 statistical children service neighbours with the lowest percentage in Stockton-on-tees at 41.1%. (Children and Maternal Health, 2020). There are no data on inequalities within Bury but England data suggests decreasing percentage of under 18 conceptions leading to abortion with increasing levels of deprivation. The most deprived decile in England has an under-18 abortion percentage of 45.7% compared with 60.2 in the least deprived decile for the year 2020 (Child and Maternal Health, 2020).
c. Risk and protective factors and health behaviours in pregnancy
Many factors affect a woman’s health in pregnancy. The extent to which these can be altered or modified varies. For example, once a woman is pregnant, factors such as the age at which she will become a mother cannot be altered. There are, however, less healthy behaviours which are often established well before pregnancy. This is the case for dietary and exercise habits, smoking, alcohol and substance misuse and many other factors. Effective action to reduce these risk factors before and during pregnancy can improve outcomes for mothers, babies and their families. As with many aspects of public health, inequalities in maternal and infant outcomes exist, with poorer outcomes experienced by certain groups of women and their babies. These risk factors and the health behaviours will be presented next.
Folic acid supplements before pregnancy
Folic acid (also known as vitamin B9) is essential for the development of a healthy foetus because it reduces the risk of neural tube defects (NTDs) like spina bifida. Percentage of pregnant women who started taking folic acid prior to pregnancy as reported at time of booking appointment with midwife in Bury (19.1%) is lower (statistically significant) than 27.3% in England. No trend data are available for Bury and England. Bury has the lowest percentage of women taking folic acid supplements in its group of children's services statistical neighbours, with the highest uptake in Stockport of 35% (Sexual & reproductive health profiles, 2021).
Smoking
Smoking during pregnancy is associated with a variety of adverse birth outcomes including low birth weight and preterm birth, increased risk of stillbirths, placental problems, restricted head growth and an increased risk of miscarriage. Health and developmental consequences among children have also been linked to prenatal smoke exposure, including poorer lung function, persistent wheezing, and asthma, possibly through DNA methylation and visual difficulties, such as strabismus, refractive errors, and retinopathy.
Smoking in early pregnancy
Based on the most recent data from 2018-19, 11.1% of pregnant women in Bury smoked at the time of booking appointment with midwife, lower (statistically significant) than 12.8% in England. No trend data are available for Bury and England. Bury has the 2nd lowest percentage of pregnant women smoking at the time of booking appointment with midwife in its group of children's services statistical neighbours, with the lowest percentage in Stockport of 10.8% and highest in Calderdale at 19.6%.
Smoking status at time of delivery
This indicator is defined as the number of mothers known to be smokers at the time of delivery as a percentage of all maternities with known smoking status. A maternity is defined as a pregnant woman who gives birth to one or more live or stillborn babies of at least 24 weeks gestation, where the baby is delivered by either a midwife or doctor at home or in a NHS hospital.
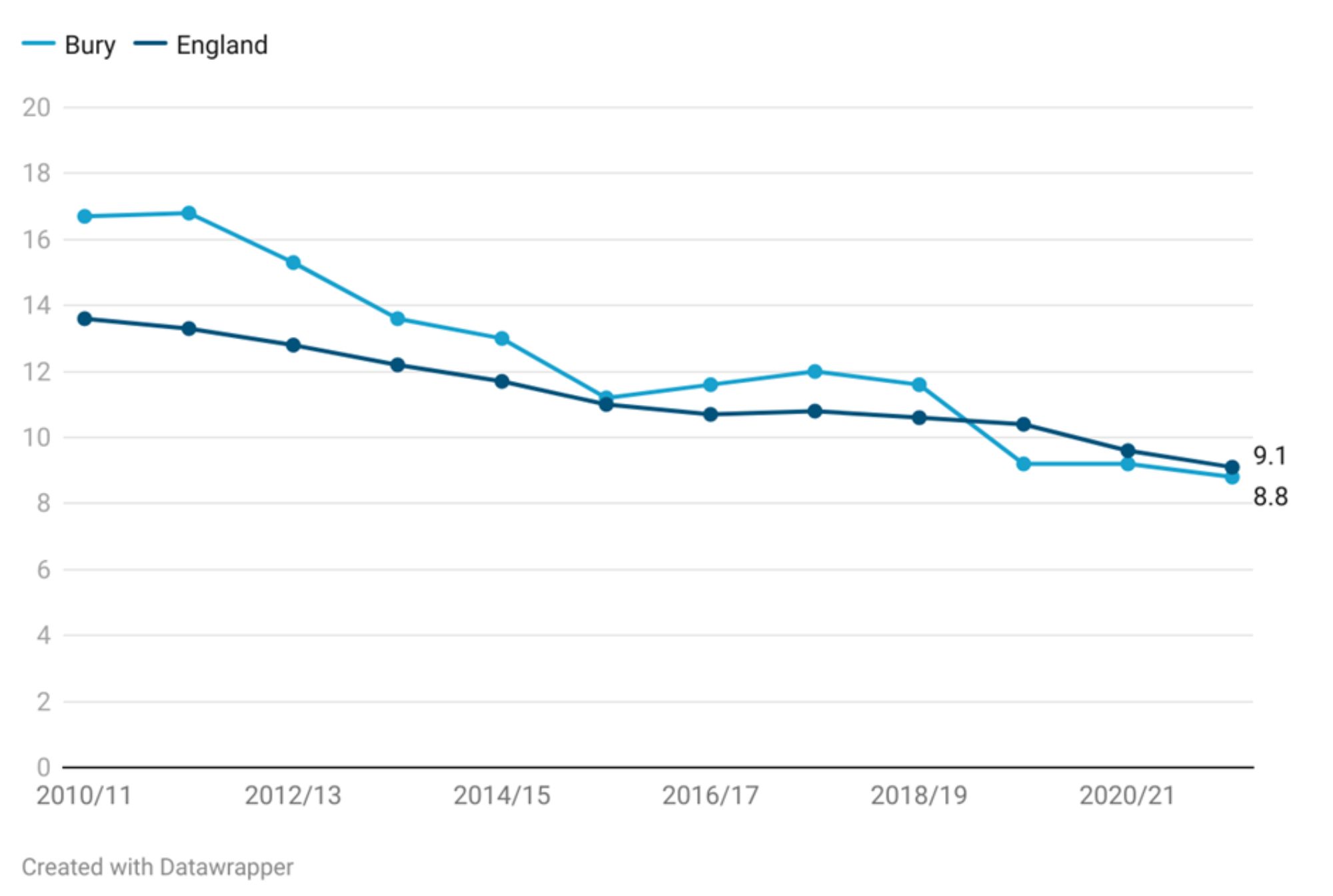
Percentage of women who were known smokers at time of delivery has declined in Bury and England over the past decade. In Bury, the percentage of women smoking at the time of delivery was 16.7% in 2010-11 (statistically higher than England average of 13.6%), steadily declining to 8.8% in 2021-22 (statistically similar to England average of 9.1%). A decrease in Bury has been seen but at a slower rate with the decline in Bury of 7.9% from 2010-11 to 201-22 and the decline in England of 4.5% during the same time period (Figure 5)
Figure 5: Comparison of smoking status at time of delivery during the period 2010-11 to 2021-22 for Bury and England
Bury has the 2nd lowest percentage (%) of women who are known smokers at the time of delivery in its group of children's services statistical neighbours in 2021 (with a statistically significant decreasing trend). The highest percentage is in Stockton-on-Tees at 14% and lowest in Stockport at 6.9% (Sexual & reproductive health profiles, 2021). There are no data on inequalities at Bury and England level.
Alcohol
There are no data on alcohol use during pregnancy for Bury and its statistical neighbours. However, data for England is available for early pregnancy that shows around 4.1% of pregnant women were recorded as drinking alcohol at the time of booking appointment with midwife in 2018-19. Data on inequalities are available for England only. Higher percentage of women (5%) in least deprived deciles in England drink in early pregnancy compared with the most deprived decile (3.3%). By ethnic groups, the highest percentage of women drinking during early pregnancy were White (4.6%), followed by mixed (4%), black (3.6) and the lowest percentage is Asian (1.8%). Examining data by age of mother for England, as the age of women increases, the percentage of women drinking in early pregnancy increases. Higher proportion of women over 45 years of age (5.6%) drink alcohol in early pregnancy compared with those under 30 years of age (3.6%). Lower proportion of women who are first time mothers drink during pregnancy (3.6%) compared with those who have a subsequent pregnancy (4.4%).
Drug misuse
There are no data on drug misuse during pregnancy for Bury and its statistical neighbours. Data for England is available for drug misuse in early pregnancy and the data suggests that 1.4% of pregnant women were recorded as misusing non-medicinal drugs or other unauthorised substances at the time of booking appointment with midwife in 2018-19. Data on inequalities are available for England only. Higher percentage of women (2.8%) in most deprived deciles in England misuse drugs in early pregnancy compared with the least deprived decile (0.4%). By ethnic groups, the highest percentage of women misusing drugs in early pregnancy were mixed (2.7%), followed by black (1.7%), white (1.4%) and the lowest percentage is Asian (1.2%). Examining data by age of mother for England, as the age of women decreases, the percentage of women misuse drugs in early pregnancy increase. Highest proportion of women under 18 years of age (3.1%) misuse drugs in early pregnancy compared with those over 45 years of age (1.5%). Lower proportion of women who are first time mothers misuse drugs in early pregnancy (1.2%) compared with those who have a subsequent pregnancy (1.4%).
Obesity
Obesity during pregnancy is measured in fingertips as percentage of pregnant women who are obese (BMI>=30kg/m2) at the time of booking appointment with midwife. Based on the most recent data from 2018-19, 22.6% of pregnant women in Bury were obese, statistically similar to England average of 22.1%. No trend data are available for Bury and England. Bury has the 3rd highest percentage of pregnant women who are classified as obese in its group of children's services statistical neighbours, with the lowest percentage in Stockport of 20.1% and highest in Calderdale at 24.9%.
d. Maternal Infectious Disease Screening
Infectious diseases in pregnancy screening (IDPS) offers and recommends screening tests for infectious diseases in pregnancy. The tests are aimed to protect maternal health through early treatment and care, reduce any risk of perinatal transmission and transmission to partner and/or other family members. The three diseases covered by IDPS are HIV, Syphilis and Hepatitis B. There are no publicly available data from IDPS on maternal infectious disease screening.
e. Maternal health care access
Early access to maternity care enables health care providers to identify and treat potential health problems in the mother and infant, resulting in better health outcomes. Early access to maternity care can also help reduce the risk of preterm birth, low birth weight, and other adverse pregnancy outcomes including maternal death. Inadequate use of antenatal care has been shown to be strongly independently associated with increased odds of maternal death.
The NHS offers a ‘booking-in’ appointment between 8 to 12 weeks of pregnancy. NICE recommends antenatal booking by 10 weeks of pregnancy. This appointment allows scheduling of ultrasound scan, identification of women who may need more care than usual due to medical history or social circumstances, discussion of antenatal screening, taking blood pressure and measuring the woman's height and weight, identification of risk factors such as smoking and providing support, and discussion of the woman's mood and mental health. It also ensures that the mother's information can be shared in a timely manner with the health visiting service, who visits the mother at home during the last three months of her pregnancy to promote health and wellbeing, plan for parenthood, and, if necessary, arrange for more intensive postpartum support.
Pregnancies booked at or after 12 weeks are considered ‘late booked’, and late booking is considered a modifiable risk factor for infant mortality. Women booking after 20 weeks of pregnancy are considered at particularly high risk because they have missed the screening window for certain infectious diseases, inherited conditions, and Down's, Edwards, and Patau's syndromes.
Early access to maternity care
Early access to maternity care is measured as the percentage of pregnant women who have their booking appointment with a midwife within 10 completed weeks of their pregnancy. The most recent data for Bury is available for the year 2018-19, where only 29.4% of women had their booking appointment within 10 completed weeks of pregnancy. This was statistically lower than England average of 57.8% (Children and Maternal Health, 2019). No trend data are available for Bury and England. Among Bury’s group of closest children's services statistical neighbours, Bury had the lowest percentage in terms of early access to maternity care, with the highest access in Calderdale at 79.2% (Children and Maternal Health, 2019). Bury’s early access to maternity care is the lowest in all of Northwest.
2. Newborn health and Birth Outcomes
Maternal health is a resource for life and ensures the best start of life for a child. Pregnancy and birth outcomes measure the health and well-being of mothers and babies during and after pregnancy and childbirth. Examining data on these outcomes allows valuable insights into the quality and accessibility of maternal and child healthcare services, as well as broader social and economic determinants of health. Publicly available data on pregnancy and birth outcomes for Bury are presented next.
a. Caesarean Section
Caesarean sections (commonly referred to as c-sections) are often required for several maternal and infant reasons. By their nature (i.e. they are used when there are complications) they are likely to be associated with an increased risk of problems.
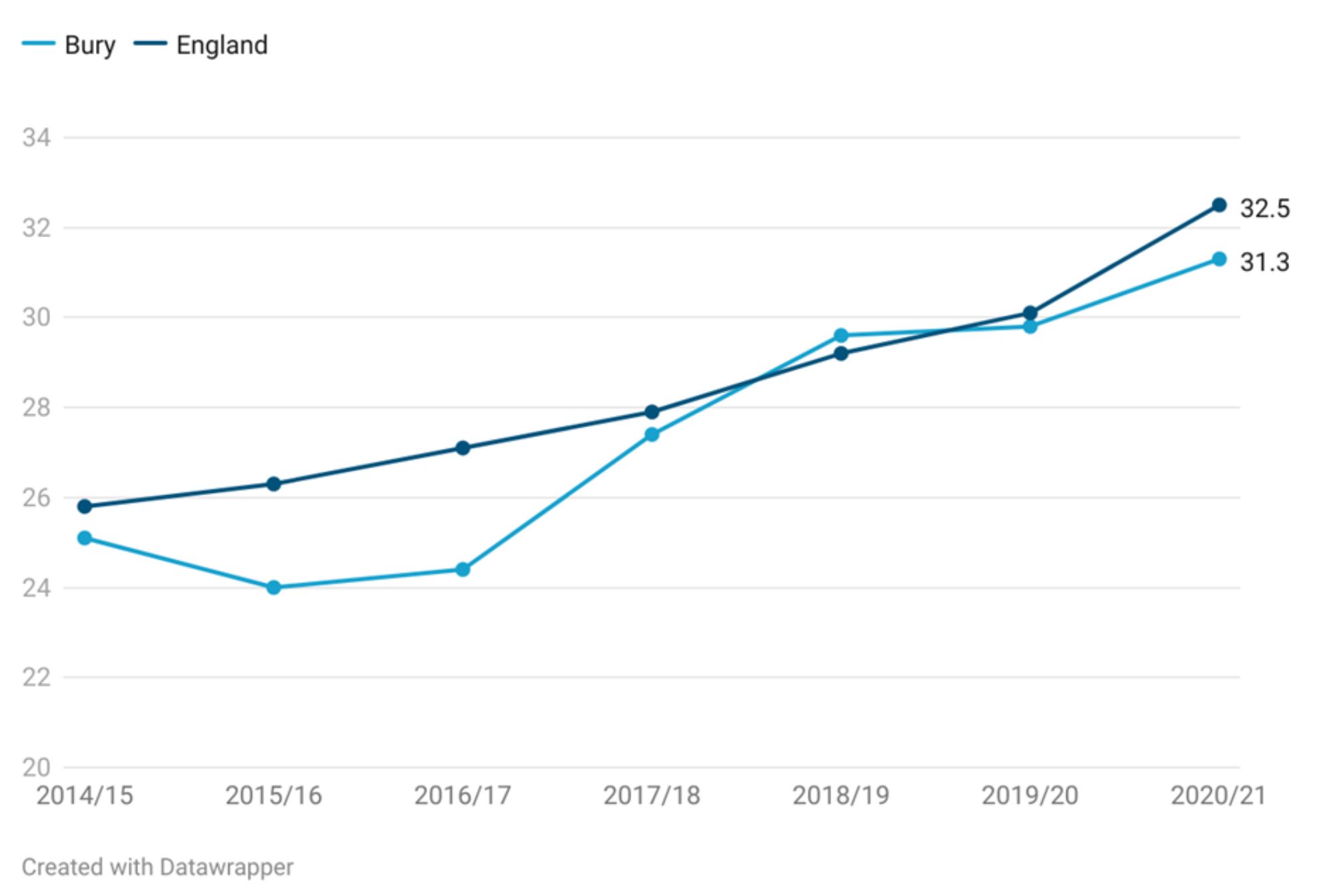
There has been an increase in percentage of caesarean sections in Bury and England from 2014-15 to 2020-21, with a particularly rapid increase from 2017/18 to 2020/21. In Bury, the percentage of women who had a c-section increased by 6.2% from 25.1% in 2014-15 compared with 31.3% in 2020-21 (statistically similar to England average). % The percentage of c-sections in England has also been increasing over the same period, with an increase of 6.7%, from 25.8% in 2014-15 to 32.5% in 2020-21. The percentage of c-sections in Bury have remained lower than England average (in terms of percentage), apart from 2018-19, where the percentage of c-sections in Bury were slightly higher (29.6%) compared with England (29.2%). The gap in percentage of c-sections between Bury and England has fluctuated with the largest gap of 2.7% in 2016-17 (24.4% in Bury vs 27.1% in England) (Figure 6)
Figure 6: Comparison of percentage of c-sections during the period 2014-15 to 2020-21 for Bury and England
Bury has the 4th highest percentage (%) of c-sections in its group of children's services statistical neighbours in 2020-21. The highest percentage is in Stockport at 35.9% and lowest in Calderdale at 27.4% (Children and Maternal Health, 2021). There are no data on inequalities at Bury level. Data at the national level suggests that as the levels of deprivation decreases, the percentage of c-sections increase. The percentage of c-section in the most deprived decile in England is 30.2% compared with 33.5% in the least deprived decile (Child and Maternal Health, 2021).
b. Premature births (less than 37 weeks gestation)
The World Health Organization (WHO) defines premature births (also referred as preterm births) as babies born alive before 37 weeks of pregnancy are completed (WHO, 2022). Babies may be born prematurely due to spontaneous preterm labour or a medical indication to schedule an induction of labour or caesarean birth early. Premature births can lead to low birth weight that is closely associated with foetal and neonatal mortality and morbidity, stunted growth and cognitive development, and NCDs later in life, among other negative health outcomes.
There is strong evidence that smoking while pregnant and exposure to second-hand smoke can result in premature birth, in addition to many other adverse health effects, such as complications during labour, low birth weight at full term, and an increased risk of miscarriage and stillbirth (Child and Maternal Health, 2020).
Premature births are measured in fingertips as crude rate of premature live births (gestational age between 24-36 weeks) and all stillbirths per 1,000 live births and stillbirths.
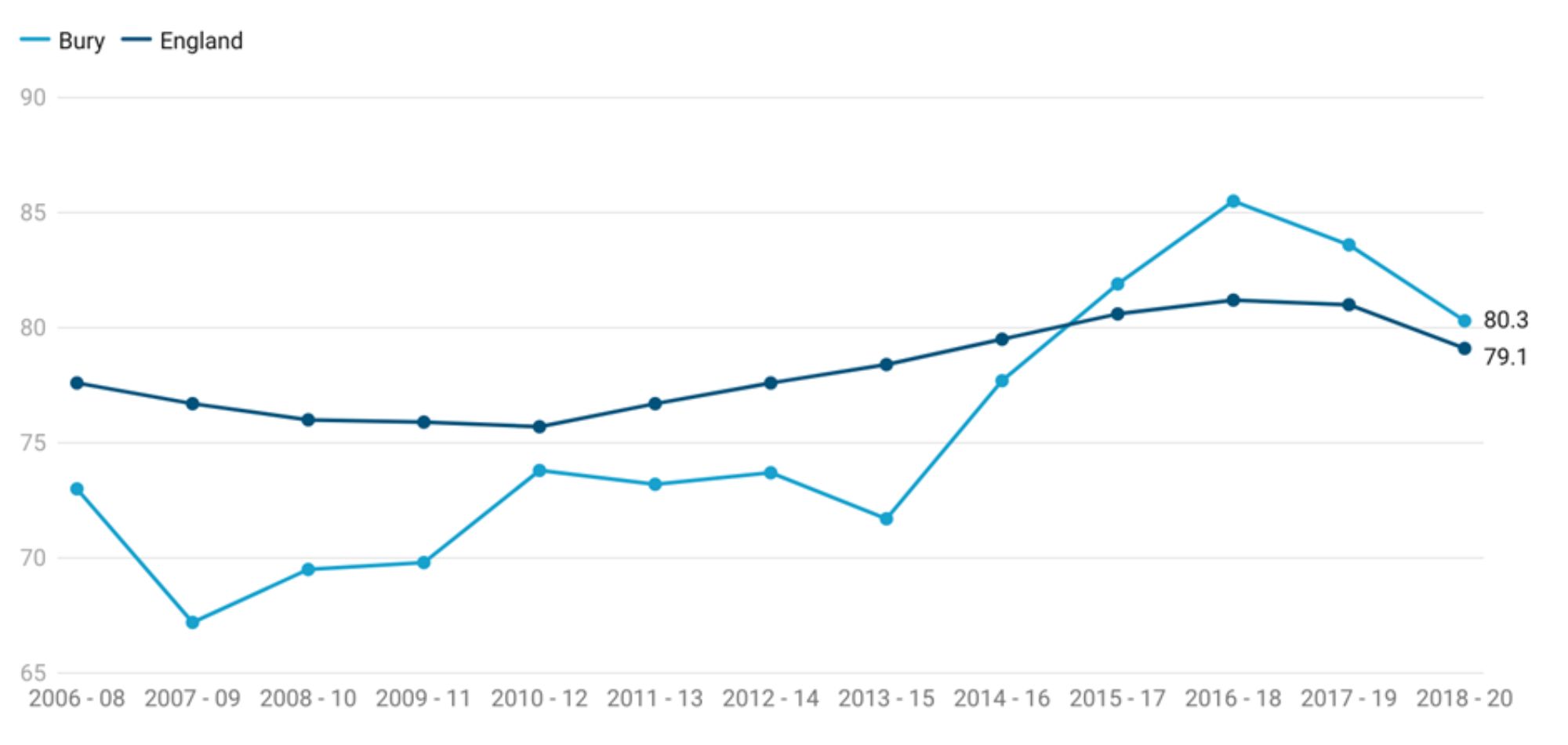
Premature births in Bury have been fluctuating in Bury throughout the period 2006-08 to 2018-20. From the period 2006-08 to 2013-15, premature birth rates in Bury were stable, ranging from a rate of 67.2 to 73.8 per 1,000 live births and stillbirths. From 2013-15 to 2016-18, the premature birth rates in Bury increased rapidly, from 71.7 to 85.5 per 1,000 live births and stillbirths. In the most recent period (2018-20), the premature birth rate in Bury has declined to 80.3 per 1,000 live births and stillbirths. Throughout the period 2006-08 to 2014-16, premature birth rate in Bury remained below the average for England (although only statistically significant lower for the period 2007-09, 2008-10 and 2013-15). From 2015-17 to 2018-20, the rates in Bury were higher than England average but were not statistically significant.
Similar to Bury, the premature birth rate in England has been fluctuating over time, with some periods of increase and some periods of decrease. During the period 2006-08 to 2010-12, premature birth rate in England decreased gradually from 77.6 to 75.7 per 1,000 live births and stillbirths. From 2010-12 to 2016-18, the premature birth rate in England increased to 81.2 per 1,000 live births and stillbirths. In the most recent period (2018-20), there has been a slight decline to 79.1 per 1,000 live births and stillbirths.
Premature birth rate in Bury has shown a more rapid increase in recent years than in England, but the most recent data for both areas show a decrease in premature birth rate (Figure 7)
Figure 7: Comparison of crude rate of premature live births (gestational age between 24-36 weeks) and all stillbirths per 1,000 live births and stillbirths during the period 2006-08 to 2018-20 for Bury and England
Bury has the 3rd highest preterm birth rates in its group of 6 statistical children service neighbours with the lowest rate in Stockport of 78.9 and highest in Lancashire of 83.6. (Children and Maternal Health, 2020). There are no data on inequalities at Bury level but England data suggests an increasing rate of preterm births with increasing levels of deprivation. The most deprived decile in England has preterm birth rate of 87.8 compared with 76 in the least deprived decile for the year 2020 (Child and Maternal Health, 2020).
c. Neonatal Mortality and Stillbirth rate
Preterm birth, intrapartum-related complications (birth asphyxia or inability to breathe at birth), infections and birth defects are the leading causes of most neonatal death. Children who die within the first 28 days of birth suffer from conditions and diseases associated with lack of quality care at or immediately after birth and in the first days of life. Neonatal Mortality and Stillbirth rate is measured as a crude rate based on the number of stillbirths and deaths under 28 days, per 1,000 live births and stillbirths.
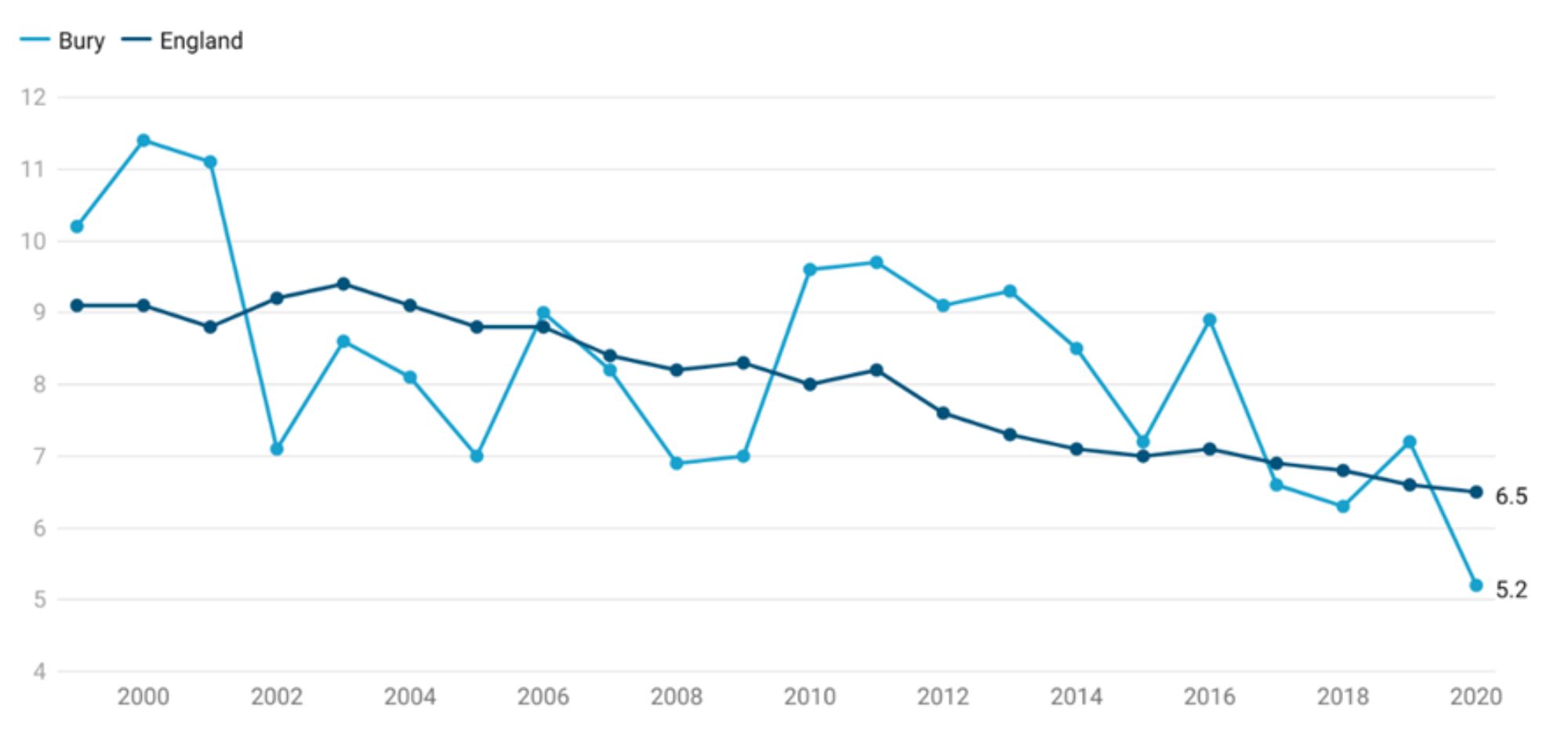
Neonatal mortality and stillbirth crude rate in Bury has fluctuated over the years. However, there has been an overall decline from 10.2 in the year 1999 to 5.2 per 1,000 live births and stillbirths in 2020. The highest rate in Bury was in the year 2000 at 11.4 per 1,000 live births and stillbirths declining to 7.1 in 2002. This was followed by a rise to 8.6 in 2003 and another decline till 2005, where the rate was 7 per 1,000 live births and stillbirths. Neonatal mortality and stillbirth rates increased once again to 9 in 2006 followed by a steady decline to 7 in 2009. From the year 2010 to 2020, there has been a consistent decline from 9.6 per 1,000 live births and stillbirths to 5.2 per 1,000 live births in 2020.
The neonatal mortality and stillbirth rate in England has been declining steadily (with some fluctuations) between the years 1999 and 2020. The highest rate was observed in 1999 at 9.1 per 1,000 live births and stillbirths and lowest in 2020 at 6.5 per 1,000 live births and stillbirths (Figure 8). Throughout this period, neonatal mortality and stillbirth rates remained similar (statistically significant) to England average.
Figure 8: Comparison of neonatal mortality and stillbirth crude rate per 1,000 live births and stillbirths during the period 2006-08 to 2018-20 for Bury and England
Bury has the 3rd highest neonatal mortality and stillbirth rate in its group of 6 statistical children service neighbours with the lowest rate in Stockton-on-Tees of 3.6 and highest in Lancashire of 6.7 (Children and Maternal Health, 2020). There are no data on inequalities at Bury level but England data suggests an increasing neonatal mortality and stillbirth rate with increasing levels of deprivation. The most deprived decile in England neonatal mortality and stillbirth rate of 8.7 compared with 4.7 in the least deprived decile for the year 2020 (Child and Maternal Health, 2020). Examining data by age of mother for England, the highest rate of neonatal mortality and stillbirth rate is in women aged 40 and over (8.7) and lowest in 25-29 year olds (5.5).
d. Birth weight of babies
At a population level, birth weight is an indicator of a multifaceted areas of public health importance that includes long-term maternal nutrition, health and health care in pregnancy. Birth weight or size at birth is an important indicator of the child's vulnerability to the risk of childhood illnesses and diseases. Birth weight also predicts the child's future health, growth, psychosocial development, and chances of survival.
Fingertips presents data on low birth weight for babies at term and all babies. Low birth weight has been defined by WHO as weight at birth of < 2500 grams (5.5 pounds). The causes of low birth weight are intrauterine growth restriction (IUGR), premature birth, or both. It is closely associated with foetal and neonatal mortality and morbidity, stunted growth and cognitive development, and NCDs later in life, among other negative health outcomes. Infants with a low birth weight are approximately 20 times more likely to die than heavier infants (WHO, 2018).
Low birth weight of all babies
Low birth weight (LBW) of all babies is defined as all births (live and stillbirths) with a recorded birth weight under 2500g as a percentage of all live births with stated birth weight, regardless of the gestational age of the baby when born.
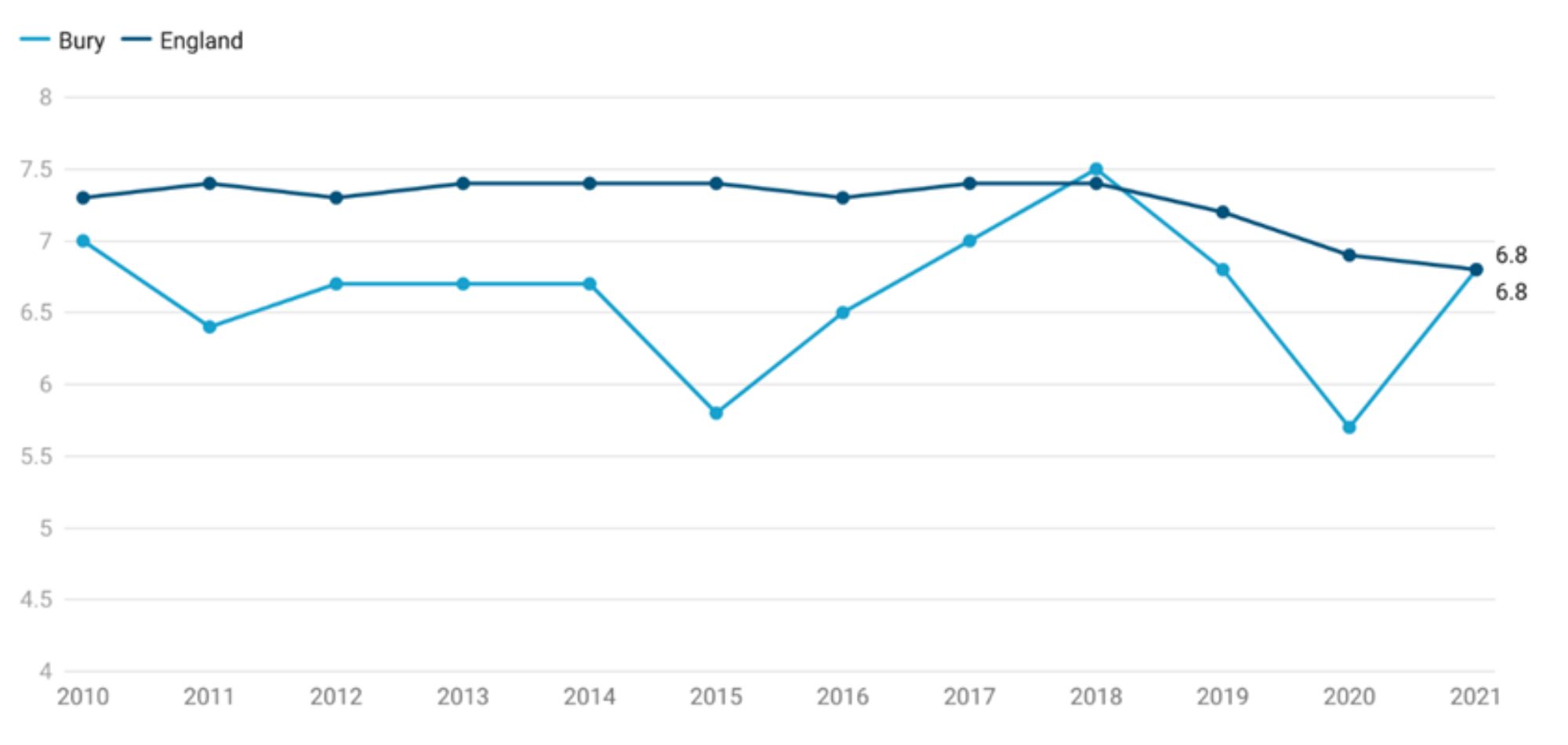
Data for Bury shows fluctuations with some slight increases and decreases. From the year 2010 to 2015, percentage of all babies with LBW declined from 7% to 5%. This was followed by a rise to 6.5% in 2016, steadily increased to 7.5% in 2018 and declining once again to 5.7% in 2019. Most recent data show another increase in LBW in all babies to 6.8% in 2021. The proportion for Bury has remained statistically similar to England average throughout this time period, apart from 2018 (5.8% in Bury vs 7.4% in England) and 2020 (5.7% in Bury vs 6.9% in England), where the proportion in Bury was statistically lower than England average. The proportion of LBW in all babies in England is following a downwards trend with a slight decline from 7.3% in 2010 to 6.8% in 2021 (Figure 8).
Figure 8: Comparison of percentage of low birth weight with a recorded birth weight under 2500g as a percentage of all live births with stated birth weight for Bury and England
Bury has the 4th highest proportion of LBW in all babies in its group of 6 statistical children service neighbours with the lowest proportion in Calderdale of 6.2% and highest in Stockton-on-Tees at 8.1% (Children and Maternal Health, 2020). There are no data on inequalities at Bury level but England data suggests a sharp deprivation gradient with increasing proportion of LBW in all babies as the levels of deprivation increases. The most deprived decile in England has 9% of LBW in all babies compared with 5.3% in the least deprived decile for the year 2021 (Child and Maternal Health, 2020).
Low birth weight of term babies
This indicator is consistent with the government's direction for public health, which emphasises prevention and early intervention. It has also been incorporated into the Department of Health's business plan in the context of addressing issues of premature deaths, preventable illness, and health inequalities, especially in relation to child poverty. It is defined as live births with a recorded birth weight under 2500g and a gestational age of at least 37 complete weeks as a percentage of all live births with recorded birth weight and a gestational age of at least 37 complete weeks. Unlike the previous indicator, this excludes babies born prematurely.
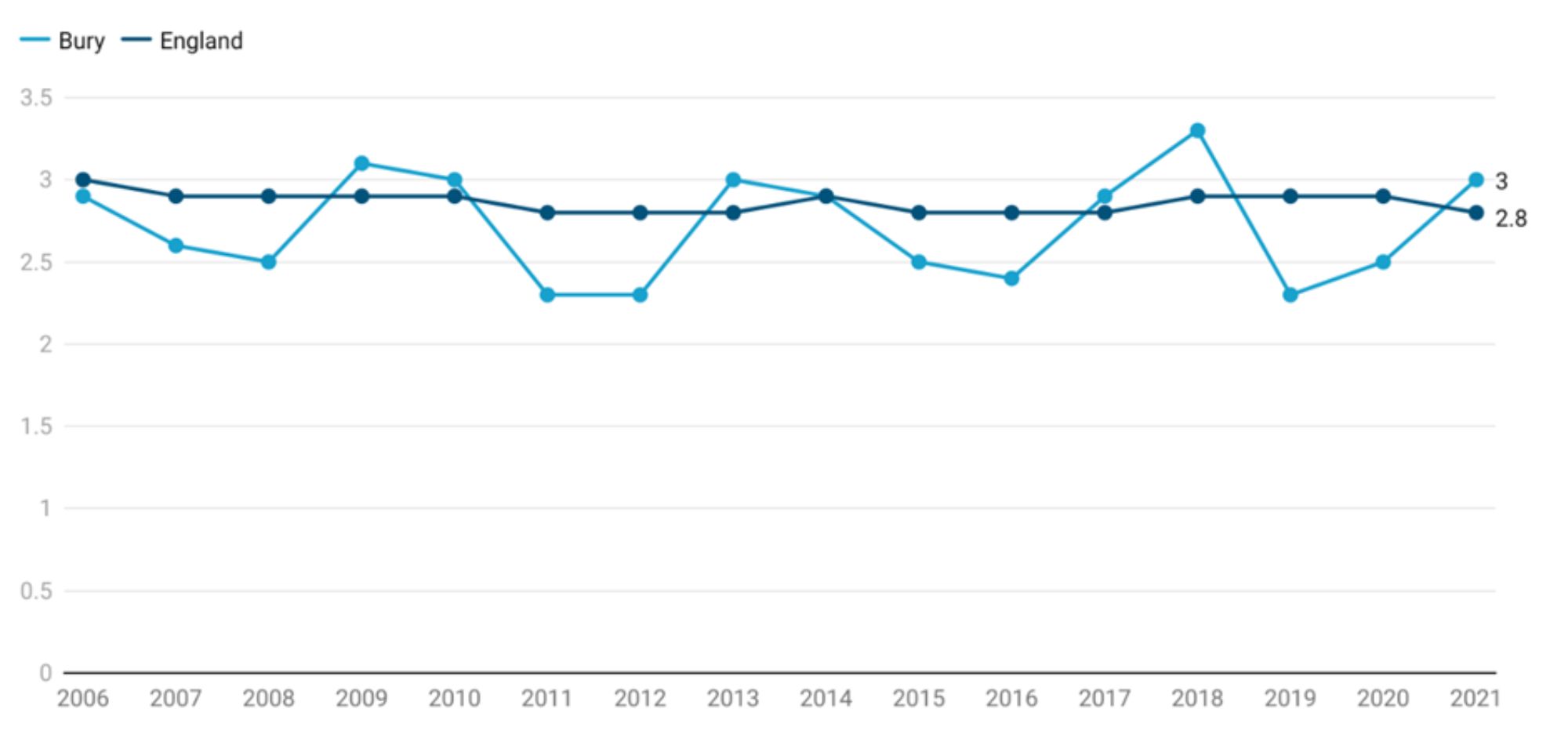
Data for Bury shows fluctuations with some small increases and decreases. There is no significant trend in Bury and the percentage of term babies with LBW increased slightly from 2.9% in 2006 to 3% in 2021. The proportion for Bury has remained statistically similar to England average throughout this time. The proportion of term babies with LBW in England has gradually declined from 3% in 2006 to 2.8% in 2021 (Figure 9).
Figure 9: Comparison of percentage of low birth weight of term babies with a recorded birth weight under 2500g and a gestational age of at least 37 complete weeks as a percentage of all live births with recorded birth weight and a gestational age of at least 37 complete weeks for Bury and England
Bury has the 3rd highest proportion of term babies with LBW in its group of statistical children service neighbours with the highest proportion in Calderdale of 3.1% and lowest in Stockport at 1.7% (Children and Maternal Health, 2020). There are no data on inequalities at Bury level but England data suggests a deprivation gradient with increasing proportion of LBW in term babies as the levels of deprivation increases. The most deprived decile in England has 3.9% of LBW in term babies compared with 2% in the least deprived decile for the year 2021 (Child and Maternal Health, 2017).
e. Low birth weight of live babies, five year pooled data
This indicator is defined as percentage of all live births with a recorded birth weight under 2500g as a percentage of all live births with stated birth weight, pooled over five years. This indicator has been included as it is available at the ward level and provides valuable insights into geographical variations in Bury.
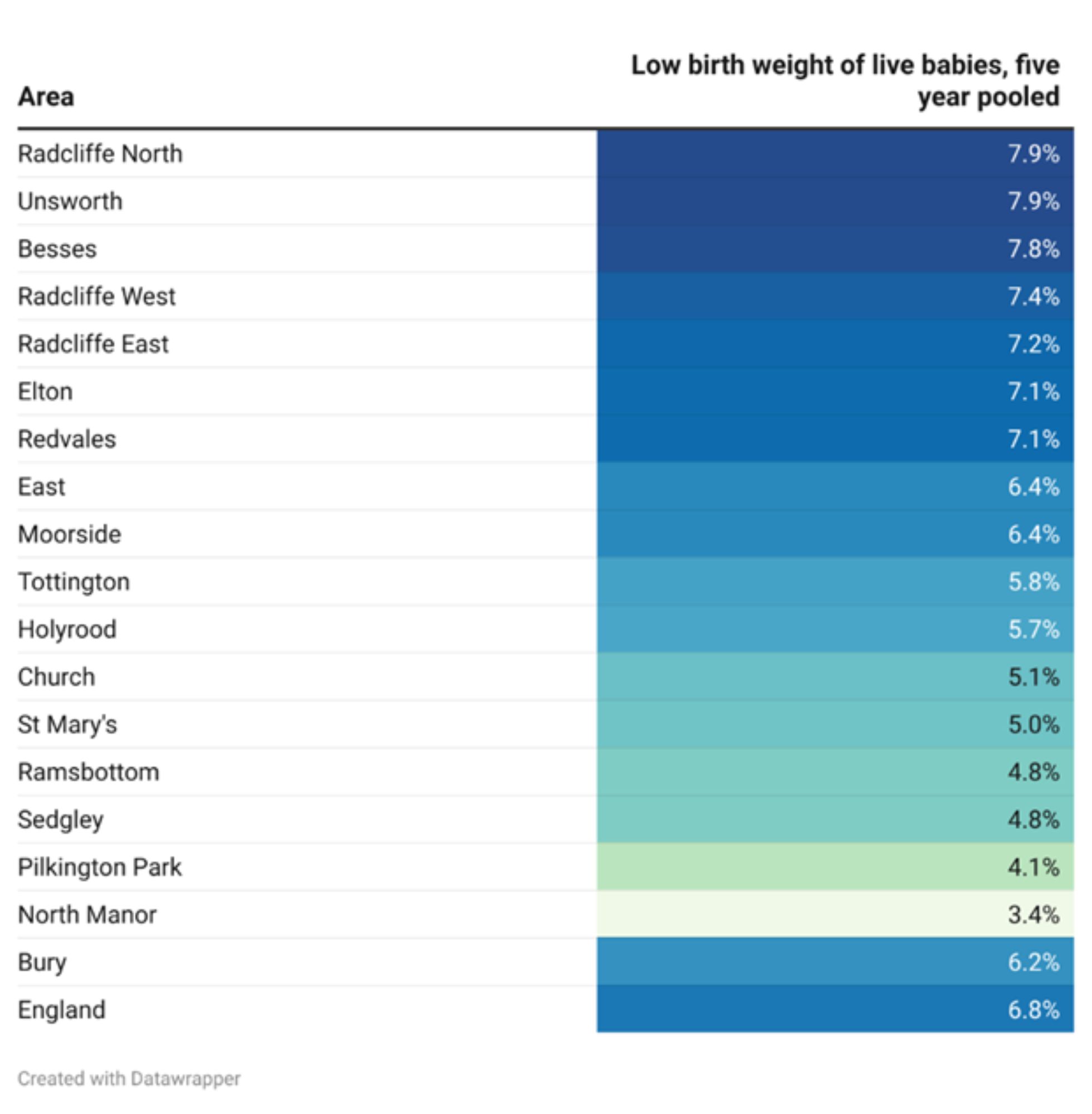
The percentage of low birth weight of live babies in Bury for the five year pooled data from 2016-20 is 6.2%, slightly lower than England average of 6.8%. Examining data by ward, the highest percentages of low birth weight of live babies are in Radcliffe North and Unsworth at 7.9% and Besses at 7.4% in the period 2016-20. The lowest percentage during the same time period is in North Manor (3.4%) and Pilkington park (4.1%) (Table 1)
Table 1: Percentage of low birth weight of live babies in Bury wards, Bury and England (five years pooled data from 2016 to 2020)
f. Multiple births
Multiple births have significantly higher rates of stillbirth, neonatal mortality, infant mortality, preterm birth, low birth weight, congenital anomalies, and subsequent developmental problems compared to single births. Each of these has implications for families and society. Multiple birth rates are affected by differences in the percentages of older women who give birth, the extent of ovarian stimulation and assisted conception, and other factors. They therefore contribute to geographical and temporal variations in infant and childhood mortality and morbidity rates.
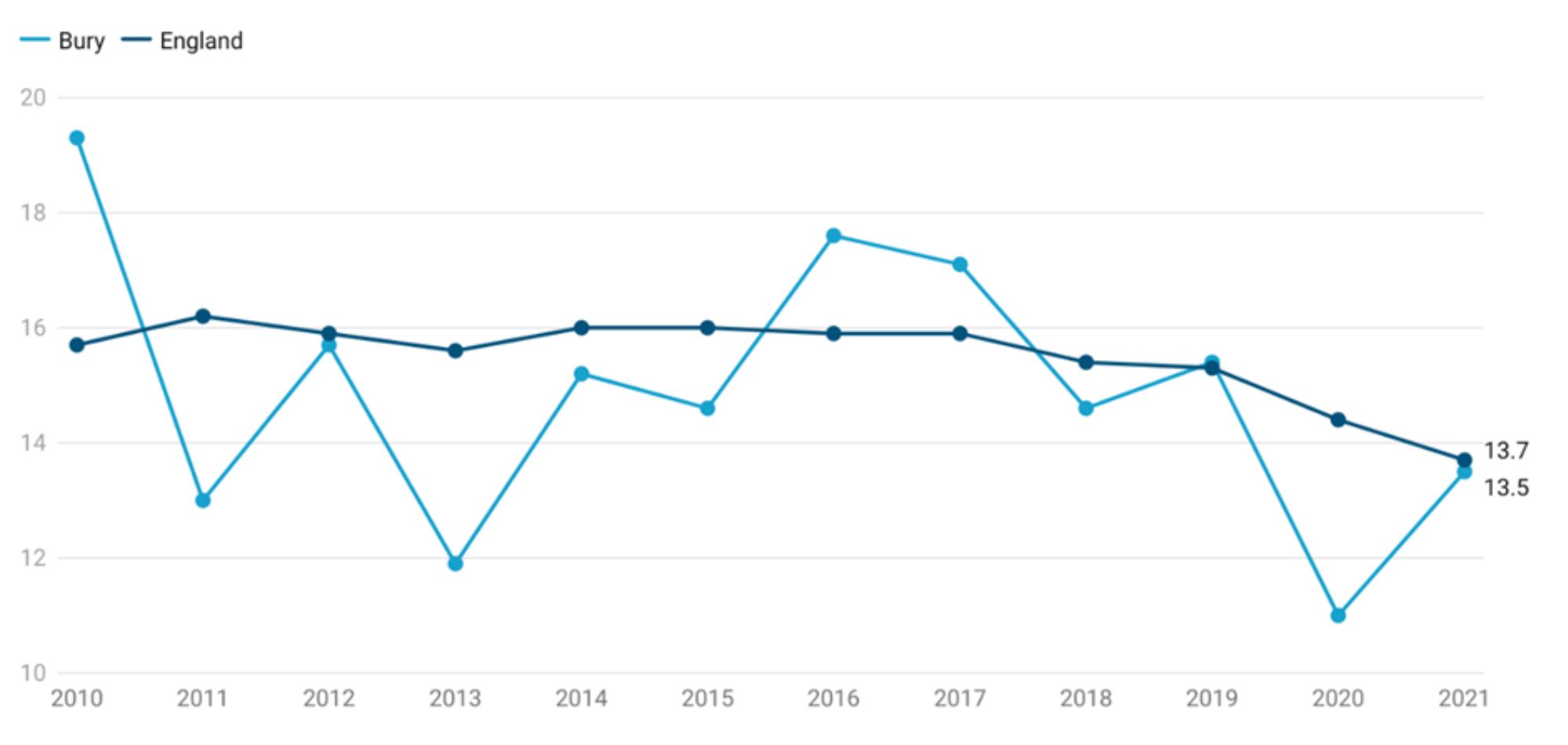
Multiple births are defined as number of maternities where the outcome is a multiple birth expressed as a rate per 1,000 total maternities. The rates in Bury have fluctuated from a high of 19.3 per 1,000 total maternities in 2010 to the lowest at 13.5 per 1,000 maternities in the year 2020. The trend in Bury shows a slight decrease in multiple birth rates between 2010 and 2021. However, data based on the five most recent data points do not show any significant change.
England has also seen slight fluctuations in the multiple birth rates between 2010 to 2021 with the highest multiple birth rate of 16.2 per 1,000 maternities in 2011 and lowest of 13.7 per 1,000 maternities in 2021. England has a decreasing trend in multiple birth rates based on the 5 most recent data points. (Figure 10).
Figure 10: Comparison of rate of multiple births per 1,000 total maternities for Bury and England
Bury has the 3rd highest multiple birth rates in its group of statistical children service neighbours with the lowest rate in Calderdale of 8.9 per 1,000 maternities and highest in Stockport at 15 per 1,000 maternities (Children and Maternal Health, 2021). There are no data on inequalities at Bury level but England data suggests a slight deprivation gradient. The most deprived decile in England has the lowest multiple birth rates at 12.4 per 1,000 maternities and the least deprived decile has the highest multiple birth rates at 15.6 in the year 2021 (Child and Maternal Health, 2021).
g. Admission of babies under 14 days
High admission rates of mothers or infants shortly after birth may indicate problems with the timing or quality of health assessments before the initial transfer or with the postnatal care provided once the mother returns home. Dehydration and jaundice are two common reasons for re-admission of infants and are frequently associated with feeding difficulties.
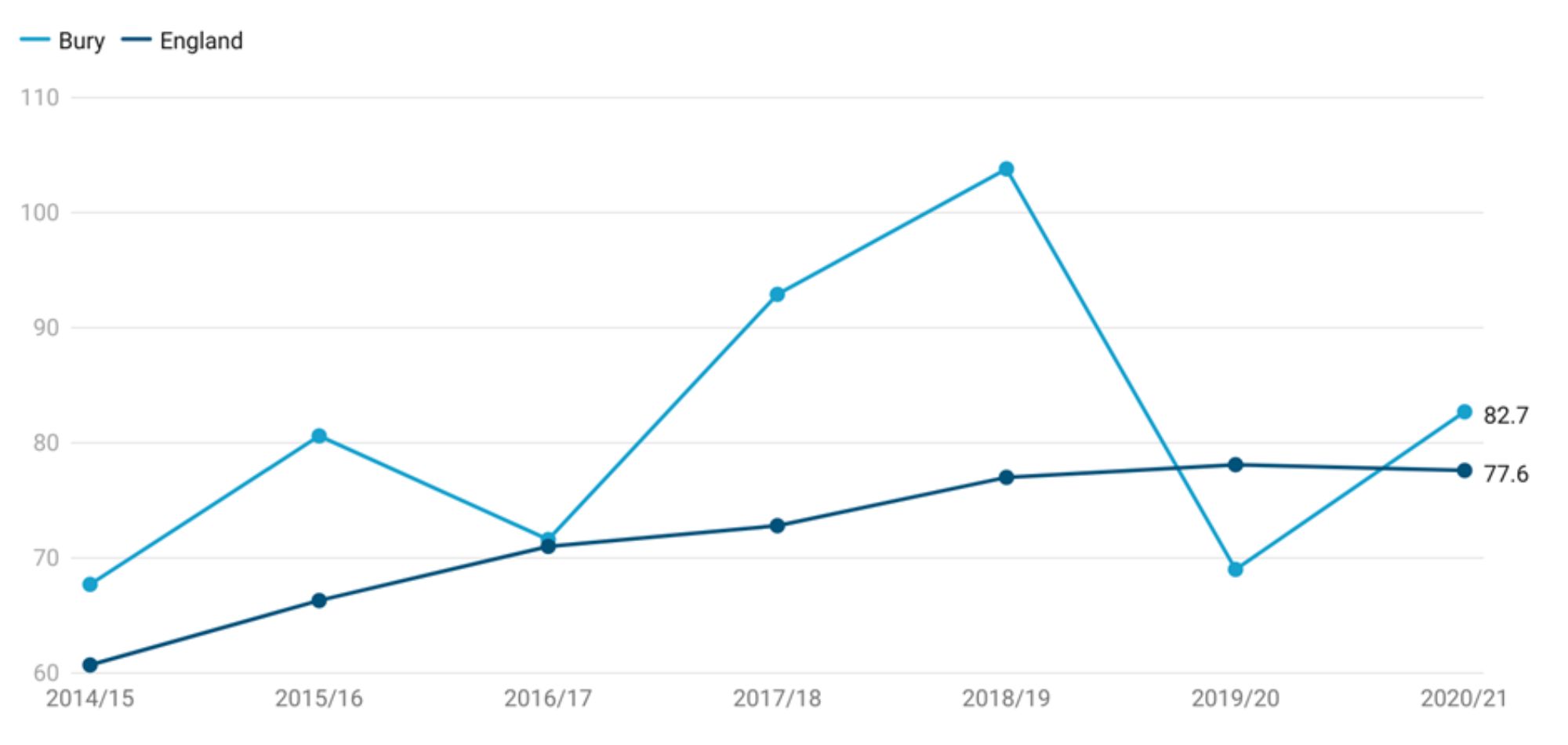
Admission of babies under 14 days are expressed as crude rates per 1,000 deliveries based on the number of emergency admissions from babies aged 0-13 days (inclusive). There are wide variations in crude admission rates for babies under 14 days in Bury, with the highest rates in 2018-19 at 103.8 per 1,000 deliveries and the lowest in 2014-15 at 67.7 per 1,000 deliveries. The admission rates in Bury increased from 67.7 in 2014-15 to 103.8 in 2018-19, followed by a decrease to 69 in 2019-20 and a slight increase to 82.7 in 2020-21. Based on the five most recent data points for Bury, there is no significant change in trend.
Admission rates in England increased from 60.7 per 1,000 deliveries in 2014-15 to the highest rate at 78.7 in 2019-20. This was followed by a slight decrease to 77.6 in 2020-21. General trend for England over the most recent data points shows that the admission rates for babies under 14 days are increasing and getting worse.
Figure 11: Comparison of crude admission rate for babies under 14 days per 1,000 deliveries for Bury and England
Bury has the 2nd lowest admission rates for babies under 14 days in its group of statistical children service neighbours with the lowest rate in Stockton-on-Tees of 70.5 per 1,000 deliveries and highest in Stockport at 129.3 per 1,000 deliveries for 2020-21 (Children and Maternal Health, 2021). There are no data on inequalities at Bury level but England data shows the lowest admission rates in the most deprived deciles, 74.4 in decile 1 and 74.5 in decile 2. The highest rates are observed in 5th (80.1), 4th (82.1), 3rd (80.5) and 2nd (81.4) least deprived deciles. The rate in the least deprived decile is 77.6 per 1,000 deliveries (Child and Maternal Health, 2021).
3. Breast feeding
Due to the dynamic and interactive nature of breastfeeding and the unique living properties of breastmilk, human infants (12 months) and young children (aged 12–36 months) are most likely to survive, grow, and develop to their full potential when they are breastfed by their mothers (Victoria et al, 2016). Breastfeeding is essential for preventing the triple burden of malnutrition, infectious diseases, and mortality, as well as reducing the risk of obesity and chronic diseases in later life (Rollins et al, 2016). Breastfed babies are at a lower risk of gastrointestinal (due to gut protective bacteria in breast milk) and respiratory tract infections. When a baby breastfeeds, the mother's body releases hormones that prevent ovulation, resulting in lactational amenorrhea, which promotes birth spacing. Additionally, breastfeeding protects the mother from chronic diseases, such as breast and ovarian cancers, type 2 diabetes, and cardiovascular disease. The substantial, positive, early-life effects of breastfeeding on infants, mothers, families, and society are sustained throughout the life course, with substantial economic benefits.
WHO recommends exclusive breastfeeding for the first six months of life, continued breastfeeding for at least the first two years, and the introduction of complementary foods at six months postpartum. Scientific Advisory Committee on Nutrition (SACN) recommends babies are exclusively breastfed until around 6 months of age and continue to be breastfed for at least the first year of life. Additionally, solid foods should not be introduced until around 6 months to benefit the child’s overall health. Yet worldwide, many mothers who can and want to breastfeed encounter numerous barriers including structural barriers such as gender inequalities, harmful socio-cultural feeding practices, income growth and urbanisation and corporate marketing practices (Escamilla et al, 2023).
a. Babies first feed breast milk
First breast feed in babies is important as the initiation and continuation of breastfeeding begins with the first feed and the feeding of colostrum. Colostrum, a mother's first milk or the 'very first food', is a sticky, yellowish substance produced by the mother soon after birth. It is ideal for the newborn - in composition, in quantity and rich in vitamins and antibodies. Colostrum contains several concentrated properties which provide a protective coating to the lining of the gut preventing bacterial transfer.
This indicator is defined as Percentage of babies whose first feed is breastmilk. No trend data are available for Bury. Data are available for the period 2020-21 that shows only 57.1% of babies first feed is breast milk. This is statistically worse than England's average of 71.7% (Maternal and Child Health, 2021).
Bury has the 3rd lowest proportion of babies with first feed breastmilk in its group of children's services statistical neighbours in 2020-21. The lowest proportion is in Lancashire at 33.5% and the highest is in Stockton-on-Tees at 92.5% (Maternal and Child Health, 2021). There are no data on inequalities at Bury level. Data at the national level suggests that as the levels of deprivation increases, the percentage of babies with first feed breastmilk decreases. The percentage of babies with first feed breastmilk in the most deprived decile in England is 55.8 compared with 82.8% in the least deprived decile in the period 2020-21 (Child and Maternal Health, 2021).
b. Breastfeeding prevalence at 6-8 weeks after birth
This indicator was included in the public health outcomes framework as it was determined to be a valid and significant indicator of public health to encourage the continued prioritisation of breastfeeding support locally. It is measured as a percentage of infants that are totally or partially breastfed at age 6-8 weeks. Totally breastfed is defined as infants who are exclusively receiving breast milk at 6-8 weeks of age - that is, they are not receiving formula milk, any other liquids or food. Partially breastfed is defined as infants who are currently receiving breast milk at 6-8 weeks of age and who are also receiving formula milk or any other liquids or food. Not at all breastfed is defined as infants who are not currently receiving any breast milk at 6-8 weeks of age. The numerator is the count of the number of infants recorded as being totally breastfed at 6-8 weeks and the number of infants recorded as being partially breastfed. The denominator is the total number of infants due a 6-8 weeks check. (PHOF, 2022).
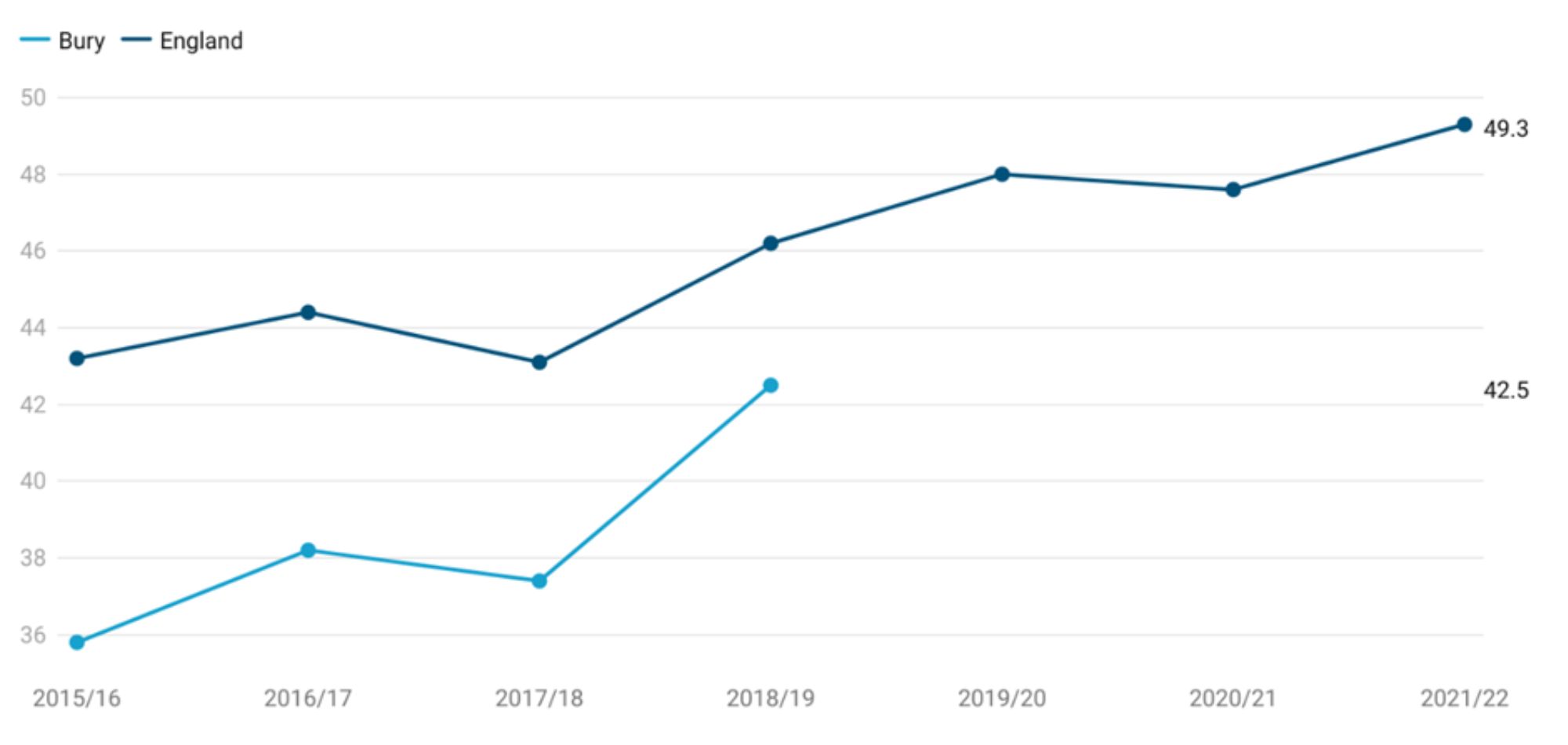
Although data for England are available from 2015-16 to 2021-22, Data for Bury are only available for the period 2015-16 to 2018-19. Breast feeding prevalence at 6-8 weeks after birth in Bury increased from 35.8% in 2015-16 to 42.5%, however remained worse (statistically significant) than England average throughout this time period. Data for England suggests an increasing trend (statistically significant) with breastfeeding prevalence at 6-8 weeks of age increasing from 43.2% in 2015-16 to 49.3% in 2021-22 (Figure 12)
Figure 12: Comparison of breastfeeding prevalence (expressed as percentage) at 6-8 weeks after birth for Bury and England (Children and Maternal Health, 2022)
Due to lack of up to date data for Bury, comparison cannot be made with its group of children's services statistical neighbours (Child and Maternal Health, 2021). There are no data on inequalities at Bury level. Data for England shows higher proportion of breastfeeding prevalence at 6-8 weeks in the least deprived decile (59.1%) compared with the most deprived decile (44.5%) (Child and Maternal Health, 2021).
c. Percentage of deliveries to mothers from Black and Minority Ethnic (BME) groups
A University of Manchester study on breast feeding rates in England found that white mothers were 69% more likely to stop breastfeeding compared with non-White mothers; they also breastfed for shorter durations compared with mothers from other ethnic groups. Other studies and surveys have shown that mothers from all minority ethnic groups are more likely to breastfeed compared with White mothers.
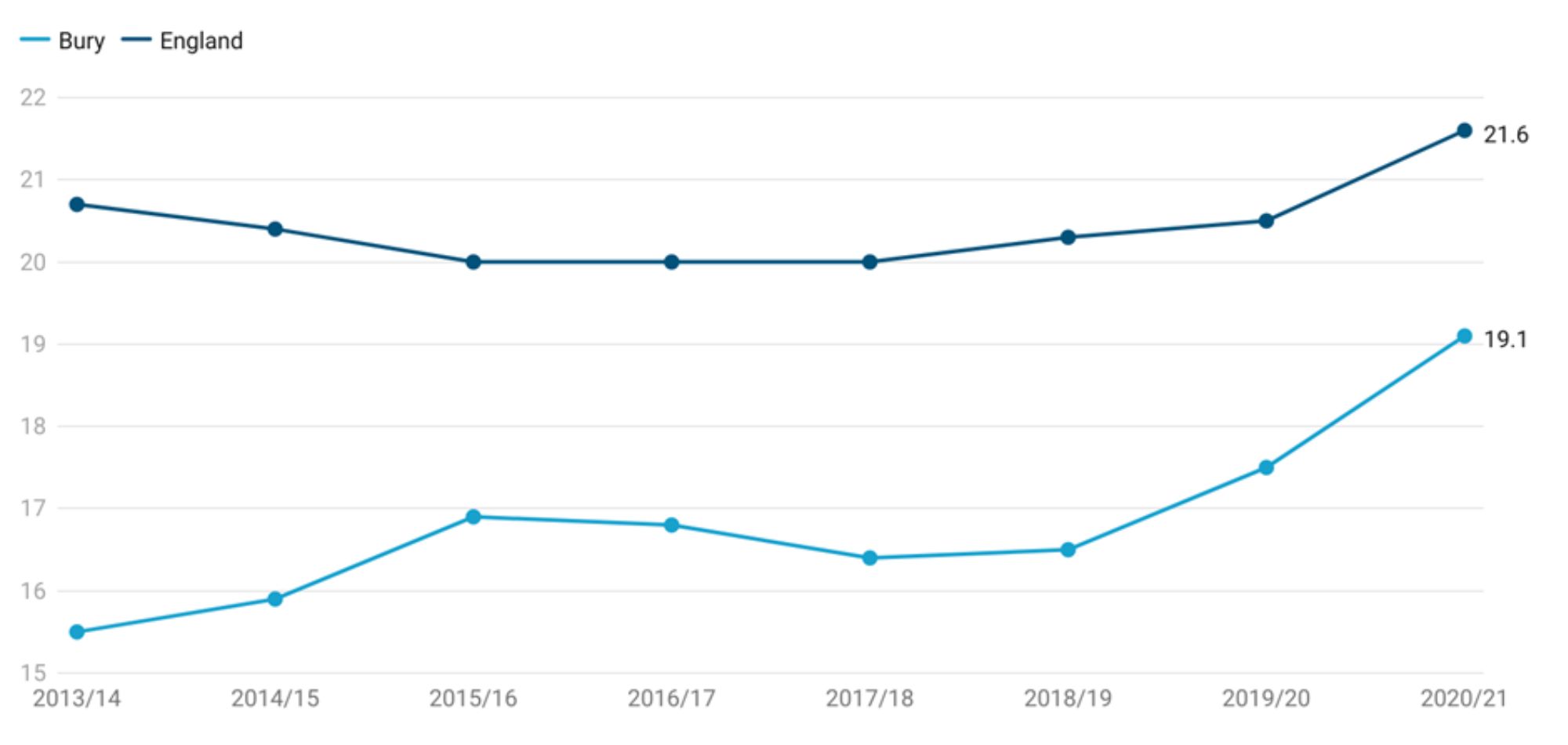
Data for Bury shows slight fluctuations with the percentage of deliveries to mothers from Black and Minority Ethnic (BME) groups increasing from 15.5% in 2013-14 to 19.1% in 2020-21. Throughout this period, the percentage in Bury has remained lower than England average. The percentage of deliveries to mothers from Black and Minority Ethnic (BME) groups increased slightly from 20.7% in 2013-14 to 21.6% in 2020-21. The increase in Bury (3.6%) has been greater than the increase for England (0.9%) (Figure 13) (Child and Maternal Health, 2020).
Figure 13: Comparison of percentage of deliveries to mothers from Black and Minority Ethnic (BME) groups for Bury and England
Bury has the 2nd highest percentage of deliveries to mothers from Black and Minority Ethnic (BME) groups in its group of children's services statistical neighbours in 2020-21. The lowest proportion is in Sefton at 4.2% and the highest is in Calderdale at 19.5% (Maternal and Child Health, 2021). There are no data on inequalities at Bury level. Data at the national level by LSOA deprivation deciles in England suggests a deprivation gradient with increasing percentage of deliveries to mothers from Black and Minority Ethnic (BME) groups with increasing levels of deprivation. The percentage of deliveries to mothers from Black and Minority Ethnic (BME) groups in the most deprived decile in England is 29.9% compared with 11% in the least deprived decile in the period 2020-21 (Child and Maternal Health, 2021).