Young People (aged 10-24 years)
Young People (aged 10-24 years)
Young People (aged 10-24 years)
This section of our Joint Strategic Needs Assessment (JSNA) presents a comprehensive overview of the health and wellbeing of young people in Bury, drawing on publicly available data from the Fingertips tool. The focus on young people, typically defined as those aged 10 to 24 years, is vital. This age group represents a critical stage of transition from childhood to adulthood, a period marked by significant physical, cognitive, and emotional development. The experiences, behaviours, and health outcomes during these years can have profound and lasting impacts on an individual's health and wellbeing throughout their lifespan.
Many health-related behaviours including diet, exercise, and substance use, are established during this time. By presenting and analysing data on these factors, we can identify trends and potential areas of concern, enabling us to intervene early and promote healthy behaviours. Moreover, many serious health conditions in adulthood have their roots in adolescence. Mental health problems, for instance, often first emerge in adolescence. By monitoring data on young people's mental health, we can inform early intervention strategies and prevent these conditions from becoming chronic and severe.
Please note: Data that are more relevant for understanding the health and wellbeing of school-age children and young people are presented in the section dedicated to the school year.
Demographics
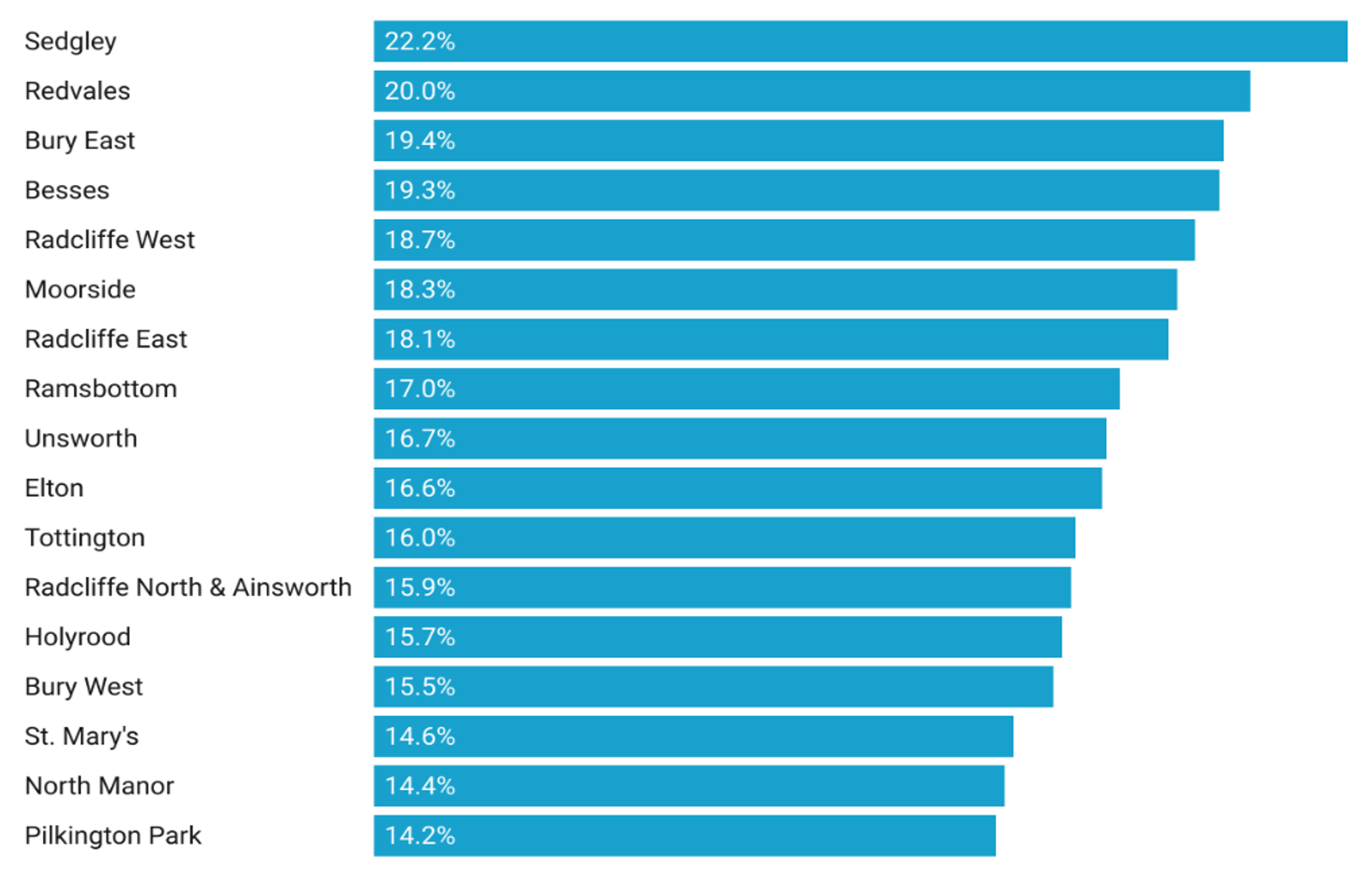
The population of young people aged 10 to 24 years in Bury is 33,628, making up 17.3% of the total population. This figure is slightly below the national average for England, which is 17.8%. The sex distribution within this demographic in Bury includes 51.5% males (17,336 individuals) and 48.5% females (16,294 individuals). When we examine the distribution of young people across different wards in Bury, Sedgley and Redvales have the highest proportions, at 22.2% and 20% respectively. In contrast, North Manor and Pilkington Park have the smallest proportions of young people, with 14.4% and 14.2% respectively.
Figure 1, presented below, offers a detailed representation of the proportion of young people (aged 10-24 years) residing in each ward in Bury, expressed as a percentage of the total population within the respective ward.
Figure 1: Proportion of young people (aged 10-24 years) living in each ward in Bury as a percentage of the total population in that ward
Education, Employment & Training
Young individuals not in education, employment, or training (NEET) face a higher risk of adverse outcomes, including health complications, mental health conditions such as depression, and early parenthood. Examining this indicator can assist us in developing a more collaborative approach among various services, with the aim of supporting young people—especially the most vulnerable—in their pursuit of education, training, and employment opportunities.
The government's strategy underscores the importance of increasing the participation of young people in learning and employment. This approach not only brings about substantial improvements to individual lives but is also a key component of the government's broader objectives to enhance social mobility and stimulate economic growth.
In a strategic move to encourage more young people to engage in studies, acquire skills and qualifications that lead to sustainable employment, and to decrease the likelihood of young individuals becoming NEET, the Education and Skills Act 2008 introduced legislation in 2013 to raise the participation age. This legislation mandates that all young people must remain in some form of education or training until the end of the academic year in which they turn 17.
As of September 2016, the Department for Education (DfE) has revised the requirement for authorities to monitor academic age 18-year-olds. Local authorities (LAs) are now only required to track and report information about young people up to the end of the academic year in which they turn 18, i.e., academic age 16 and 17-year-olds. This adjustment reflects an ongoing commitment to focus resources where they are most needed and can have the most significant impact (Child and Maternal Health, 2022).
16 to 17 year olds not in education, employment or training (NEET) or whose activity is not known.
This indicator is defined as the proportion of 16 to 17 year olds not in education, employment or training (NEET) or whose activity is not known.
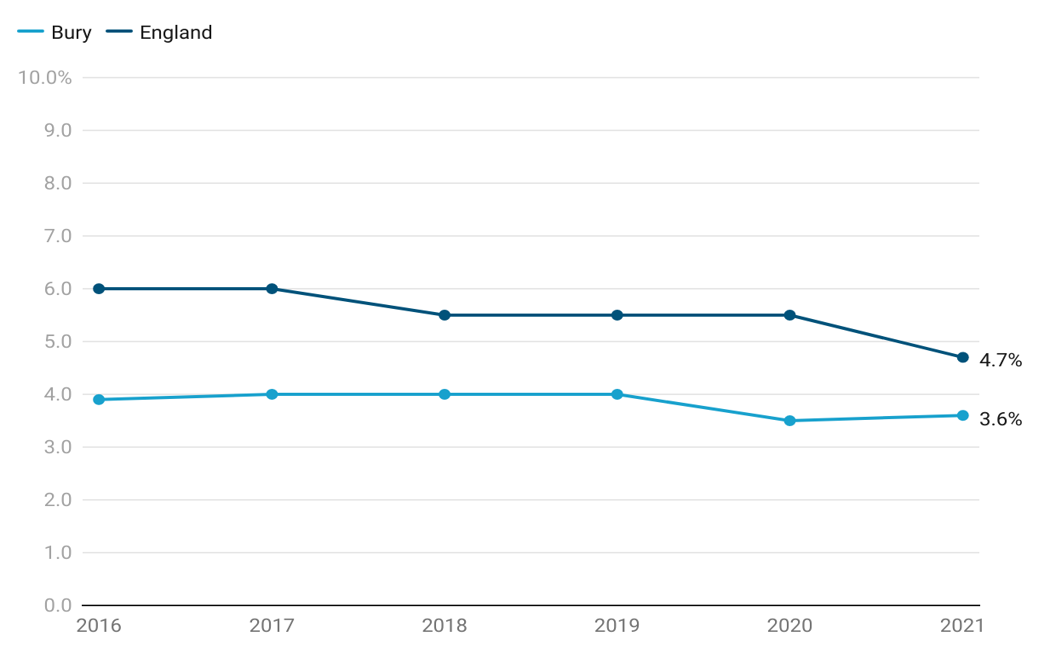
In Bury, the proportion of individuals aged 16 to 17 years who are not engaged in education, employment, or training (NEET), or whose current activity status is unknown, is 3.6%. This figure is lower (statistically significant) than the England average of 4.7%.
Over the period 2016 to 2021, the proportion of 16 to 17 year olds not in education, employment, or training (NEET) or whose activity is not known in Bury has shown some fluctuations. In 2016, the NEET proportion was 3.9%, which remained relatively stable at 4.0% in the years 2017 to 2019. In 2020, there was a slight decrease to 3.5%. The most recent data available for 2021 indicates a slight increase to 3.6%.
Examining trend data for Bury from 2006/07 to 2021/22, prevalence of overweight (including obesity) gradually declined from 23% in 2006/07 to 18.5% in 2008/09. The subsequent years, however, experienced a gradual yet somewhat inconsistent upswing, punctuated by notable peaks at 24.1% in 2016/17 and 29.2% in 2020/21. However, the most recent figure indicates a decline to 23.4% in 2021/22. A data gap exists for Bury in the 2019/20 period.
There is no significant change in trend based on the 5 most recent data points in Bury.
Data at the national level shows that in 2016, the NEET proportion in England was 6.0%, which remained relatively stable at 6.0% in 2017. This was followed by a slight decrease to 5.5% in 2018. The proportion then remained stable at 5.5% in 2018 and 2019. The most recent data available for 2021 shows a further decline to 4.7%. (Child and Maternal Health, 2021).
Bury had lower NEET proportions compared to England, with NEET proportion in Bury consistently below the national average (statistically significant) throughout the observed period between 2016 to 2021.
Figure 2: Trend in proportion of individuals aged 16 to 17 years who are not engaged in education, employment, or training (NEET), or whose current activity status is unknown for Bury and England from the year 2016 to 2021
Bury has the 4th highest NEET proportion in its group of 6 statistical children service neighbours with the highest proportion in Stockton-on-Tees at 5.3% and lowest in Stockport at 2.8% (Child and Maternal Health, 2021).
Data on inequalities in Bury are available by sex only. The proportion of males not in education, employment, or training (NEET) in Bury is higher at 4.2%, compared to females at 2.8%. However, both male and female NEET proportions in Bury are statistically similar to the average NEET proportion in Bury.
Data on inequalities are available at England level by sex, ethnic groups and deprivation.
Similar to Bury, the proportion of males not in education, employment, or training (NEET) in England is higher at 5.3%, compared to females at 4.1%. When examining NEET proportions by deprivation decile in England, the data indicates that higher deprivation deciles generally have worse NEET proportions, with the most deprived decile having the highest proportion at 6.1%. However, an interesting finding is that the least deprived decile, despite its lower overall deprivation, has a higher NEET proportion at 5.3%, which is significantly worse compared to the England average.
Data by ethnicity suggests that the highest NEET proportions are in the White and Mixed ethnic groups (both at 5% and significantly worse than England average). Conversely, the ethnic groups with the lowest proportions and significantly better than England average include Chinese (1.5%), Asian (2.4%) and Black (3%).
males have a higher prevalence of 22.5% (statistically significant) compared with females (22%).
Immunisation Coverage
Immunisation coverage is the best indicator of the level of protection a population will have against vaccine preventable communicable diseases. Coverage is closely correlated with levels of disease. Monitoring coverage identifies possible drops in immunity before levels of disease rise. Previous evidence shows that highlighting vaccination programmes encourages improvements in uptake levels.
Data on immunisation relevant to young people (10-24 years) are available for Human Papilloma Virus (HPV) vaccine (one dose at 12-13 years and two doses 13-14 years) For HPV vaccine, we will present data on one dose only as the JCVI has advised move to 1 dose of HPV vaccine for adolescents. JCVI has stated that 1 dose of the vaccine is just as effective as 2 at preventing cancers caused by HPV in adolescents. Immunisations during the early years are available under the early years section of Starting Well in the Bury JSNA.
Human Papilloma Virus (HPV) Vaccine
HPV is a common infection that is spread by skin-to-skin contact, including sexual contact, which can lead to the development of cancers affecting both women and men, including the cervix, vulva, vagina, penis, anus, and oral cavity.
On the advice of the Joint Committee on Vaccination and Immunisation (JCVI), a HPV national vaccination programme was introduced in 2008, to protect adolescent females against cervical cancer. From September 2019, 12 to 13 year old males became eligible for HPV immunisation alongside females, based on JCVI advice. This was the first year that males in year 9 were offered the HPV vaccine (OHID, 2020).
Research has shown that in England cervical cancer has almost been eliminated among young women who were offered the HPV vaccine (NIHR, 2022).
Population vaccination coverage: HPV vaccination coverage for one dose (12 to 13 year old) (Female)
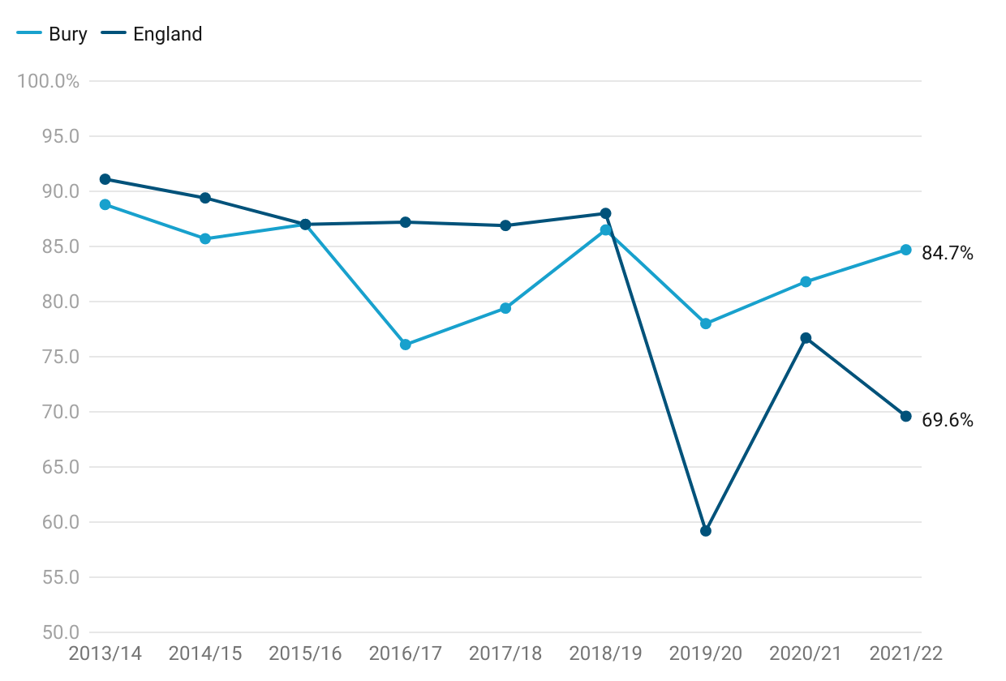
HPV vaccination coverage in Bury for one dose in females aged 12-13 years for the period 2021/22 is at 84.7%, higher than England average of 69.6% but lower than the national target of 90% or higher (Child and Maternal Health, 2022). Bury would have needed to vaccinate 57 additional females aged 12-13 years to reach the national target of 90% or higher in 2021/22.
Examining trend data for Bury from 2013/14 to 2021/22, there is a slight decrease in HPV vaccination coverage from 88.8% in 2013/14 to 85.7% in 2014/15. The coverage remains relatively stable in 2015/16 at 87%. This is followed by a drop in 2016/17 to 76.1%. The coverage then increases in 2017/18 to 79.4% and further improves in 2018/19 to 86.5%. It experiences a decline in 2019/20 to 78% but coverage has increased over the past two data points from 81.8% in 2020/21 to 84.7% in 2021/22. Throughout this period, Bury coverage has not met the national target of 90%..
England saw a gradual decline in HPV vaccination coverage (one dose) from 91.1% in 2013/14 to 86.9% in 2017/18. Coverage then remained fairly stable at 88% in 2018/19. There was a large drop in vaccination coverage in 2019/20, where it declined to 59.2% followed by an increase to 76.7% in 2020/21. The most recent data from 2021/22 suggests another decline to 69.6% in 2021/22.
Comparing Bury with England, the population vaccination coverage for HPV vaccine (one dose) was lower than England average from 2013/2014 to 2018/2019. However, in the recent years (2020/21 and 2021/22) the coverage in Bury is higher than England average (Figure 3).
Figure 3: Trend in HPV vaccination coverage for one dose (12 to 13 year old) (Female) for Bury and England from the period 2013/14 to 2021/22
Bury has the 2nd highest coverage in its group of 6 statistical children service neighbours with the highest in Stockport at 90.3% and lowest in Stockton-on-Tees at 51.4% (Child and Maternal Health, 2022).
Data on inequalities for Bury and England are only available by Sex. As we are presenting data on HPV vaccinations by males next, this comparison will not be presented here.
No geographical by PCN or GP level data are present for the HPV vaccine.
Population vaccination coverage: HPV vaccination coverage for one dose (12 to 13 year old) (Male)
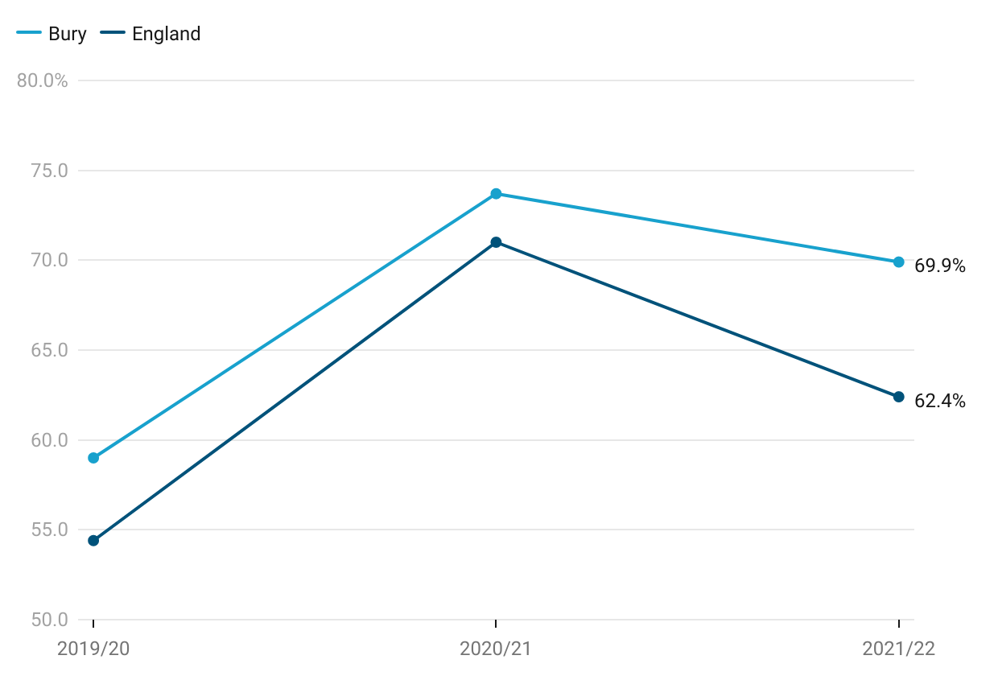
HPV vaccination coverage in Bury for one dose in males aged 12-13 years for the period 2021/22 is at 69.9%, higher than England average of 62.4% but not meeting the national target of 90% and over (Child and Maternal Health, 2022). Bury would have needed to vaccinate 250 additional males aged 12 to 13 years to reach the national target in 2021/22.
Examining trend data for Bury from 2019/20 (when HPV vaccines for males were recommended) to 2021/22, HPV vaccination coverage increased from 59% in 2019/20 to 73.7% in 2020/21. This was followed by a drop in 2021/22 to 69.9%.
England saw a fairly similar trend with coverage increasing from 54.4% in 2019/20 to 71% in 2020/21. Similar to Bury, there was a decrease in coverage to 62.4% in 2021/22.
Comparing Bury with England, the population vaccination coverage for HPV vaccine (one dose) was consistently higher than England average from 2019/20 to 2021/2022 but did not meet the national target of 90% or higher (Figure 4).
Figure 4: Trend in HPV vaccination coverage for one dose (12 to 13 year old) (Male) for Bury and England from the period 2019/20 to 2021/22
Bury has the 2nd highest coverage in its group of statistical neighbours with the highest in Stockport at 85.5% and lowest in Rochdale at 37% (Child and Maternal Health, 2022). Data are available in males by CIPFA nearest neighbours and not by children services statistical neighbours.
No geographical by PCN or GP level data are present for the HPV vaccine.
Emergency Care
This section provides data on emergency cases requiring immediate attention for young people in Bury. The data can assist in identifying gaps in care, effective resource allocation, assessment of management of diseases, informing prevention efforts and evaluating healthcare services.
Common causes for emergency hospital admissions in young people often include respiratory ailments like asthma and pneumonia, which can make them susceptible to infections. Certain chronic conditions like diabetes and epilepsy may require hospitalisation for effective management and monitoring.
Accidental injuries resulting from falls and mishaps, leading to fractures and head trauma, also contribute significantly. Moreover, mental health concerns, including self-harm and contemplation of self-harm, have emerged as crucial matters, highlighting the need for comprehensive support and assistance. Admissions from injuries and mental health concerns will be presented in their relevant sections.
Certain indicators included in the section on school-age children are also relevant to young people. Therefore, these indicators are included here to provide a comprehensive overview of the health and well-being of young individuals.
Emergency admissions (aged under 18 years)
Emergency admissions for children and young people under 18 years of age are available as crude rate per 1,000 population aged under 18 years.
Emergency admissions for children and young people under 18 years of age in Bury for period 2021/22 is 79.4, statistically higher than England average of 70.7. No trend data are available for Bury and England.
Bury has the lowest rate of emergency admissions in its group of 6 statistical children service neighbours with the highest rate in Stockton-on-Tees at 104.6 (Child and Maternal Health, 2022).
Data on inequalities for Bury are available by Sex only with higher rates in males (83.7 per 1000 and statistically worse than Bury average) compared with females (75.6 per 1000 and statistically better than Bury average) (Child and Maternal Health, 2022). England data are available by sex and levels of deprivation. Similar to Bury, males aged under 18 years have a higher admission rate (73.9 per 1000) compared with females (67.4 per 1000) Data by deprivation based on LSOA deprivation deciles suggests a deprivation gradient with increasing emergency admission rates with increasing levels of deprivation. The most deprived decile in England has an admission rate of 84.1 compared with 57.5 in the least deprived decile for the year 2021/22 (Child and Maternal Health, 2022).
A&E attendances (under 18 years)
A&E visits among children and young individuals under the age of eighteen are often avoidable and commonly caused by accidental injuries or minor illnesses that could have been treated in primary care settings. From 2008 to 2012, there were over 320,000 road-related injuries and 2,300 road fatalities involving children and young people under the age of 25 in England. In the year 2014/15, there were 19.6 million recorded attendances at major A&E departments, single specialty A&E departments, walk-in centres, and minor injury units in England. Approximately one-quarter (25.9%) of these attendances were made by children and young people aged 0-19 years.
This indicator covers A&E attendances for children as crude rates per 1000 population aged under 18 years. We have included this indicator as the age range covers school-aged children.
A&E attendances for children and young people as crude rates per 1000 population aged under 18 years under in Bury for 2021/22 is 485.5 per 1000 population aged under 18 years and statistically higher than England average of 439.8 (Child and Maternal Health, 2022).
Bury has the 4th highest rate of A&E attendance rates in its group of 6 statistical children service neighbours with the highest rate in Stockton-on-Tees of 625.1 and lowest rate in Calderdale at 418.3 for the year 2021/22 (Child and Maternal Health, 2022).
Data on inequalities for Bury are available by Sex only with higher rates in males (481.6 per 1000) compared with females (433.6 per 1000) (Child and Maternal Health, 2022). England data are available by sex and levels of deprivation. Males under 18 years of age have a higher A&E attendance rate (464.6 per 1000) compared with females (412.7 per 1000). Data by deprivation based on deprivation deciles suggests decreasing emergency admission rates with increasing levels of deprivation. The most deprived decile in England has an attendance rate of 520.9 compared with 359.9 in the least deprived decile for the year 2021-22 (Child and Maternal Health, 2022).
Asthma
Asthma is the most common chronic medical condition in children and young people in the UK (1.1 million), and it is characterised by varying levels of inflammation in the airways. Symptoms of airways inflammation include coughing, wheezing, shortness of breath, and chest tightness. Standard asthma therapies, when used regularly and correctly, can control inflammation and symptoms in most children. Having well-controlled asthma reduces the likelihood of needing hospital care.
Acute asthma episodes are preventable. Often, asthma symptoms are accepted as normal, leaving airway inflammation untreated, increasing chances of those suffering from asthma having a life-threatening asthma attack. As a result, there are increased rates of acute care episodes and preventable deaths.
Understanding local trends in emergency admissions for asthma in children and young people with this long-term condition, as well as benchmarking against geographical and statistical neighbours, will aid in service review and redesign (Child and Maternal Health, 2022).
Admissions for Asthma (10-18 years)
This indicator covers emergency admissions for asthma for young people as crude rates per 100,000 population aged 10-18 years.
Emergency admissions crude rate for asthma in young people aged 10-18 years in Bury for 2021/22 is 89.2 per 100,000 population aged 10-18 years, statistically higher than England average of 87.6 (Child and Maternal Health, 2022).
Bury has the 4th highest rate of emergency admissions for asthma in its group of 6 statistical children service neighbours with the highest rate in Stockport of 162 and lowest rate in Stockton-on-Tees at 67.3 for the year 2021-22 (Child and Maternal Health, 2022).
Data on inequalities for Bury are available for males only with statistically similar (129.2 per 100,00) to Bury average rates (Child and Maternal Health, 2022). England data are available by sex and levels of deprivation. Rates in males and females are statistically similar to average for England, however females have slightly higher rates (89.3) compared with males (86.1). Data by deprivation based on deprivation deciles suggests increasing emergency admission rates for asthma with increasing levels of deprivation. The most deprived decile in England has an admission rate of 134.4 compared with 54.6 in the least deprived decile for the year.
Diabetes
Insulin-dependent diabetes mellitus (IDDM), commonly known as type 1 diabetes, is a chronic (long-term) condition characterised by the inability of the pancreas to produce sufficient insulin. It primarily affects children and young individuals.
Effective management of insulin-dependent diabetes in children and young people plays a crucial role in preventing emergency admissions. With proper education and support, children and their families can learn to recognise and respond to warning signs and symptoms of complications. Timely monitoring of blood glucose levels, adherence to insulin regimens, and regular healthcare follow-ups are key to preventing acute episodes. Additionally, promoting healthy behaviour including a balanced diet and regular physical activity, can help maintain stable blood sugar levels and reduce the risk of emergencies. By implementing comprehensive diabetes care programs, ensuring access to necessary medications and supplies, and fostering awareness among healthcare providers, families, and schools, the occurrence of emergency admissions related to insulin-dependent diabetes in children can be significantly reduced.
Admissions for Diabetes (10-18 years)
This indicator covers emergency admissions for diabetes among young people aged 10-18 years, presenting the crude rates per 100,000 population aged 10-18 years.
For the year 2021/22, the crude rate of emergency admissions for diabetes among young people aged 10-18 years in Bury was 89.2 per 100,000 population, which is statistically similar to the England average of 80.4 (Child and Maternal Health, 2022). Bury ranks fifth in terms of emergency admissions for diabetes among its group of six statistical children service neighbours, with Stockport having the highest rate at 129.6 and Stockton-on-Tees having the lowest rate at 67.3 for the same period (Child and Maternal Health, 2022).
Data on inequalities in Bury are available by sex only. Admission rates in males and females are statistically similar to average for Bury, however females have slightly higher rates (92.4) compared with males (86.1). Data by sex in England indicates statistically lower rates in males (74.1) and statistically higher rates in females (86.9) when compared to the overall average for England. Data by deprivation based on deprivation deciles suggests increasing emergency admission rates with increasing levels of deprivation. The most deprived decile in England has an admission rate of 87.9 compared with 58.8 in the least deprived decile for the year (Child and Maternal Health, 2022).
Epilepsy
Epilepsy is a neurological condition characterised by recurring seizures. Seizures occur due to abnormal electrical activity in the brain, causing temporary disruptions in normal functioning. These seizures can present in various ways, such as convulsions, loss of consciousness, confusion, or unusual sensations. The causes of epilepsy in children and young people can be diverse, including genetic factors or brain injuries, although some cases have unknown origins. Collaborating closely with healthcare professionals is crucial for developing an individualised treatment plan, which may involve medications or other interventions to effectively manage and control seizures.
Emergency hospital admissions of children and young people aged 10-19 years with a primary diagnosis of epilepsy provides valuable insights into the management and impact of epilepsy in this age group. These admissions reveal instances where individuals with epilepsy experienced seizures that required immediate medical attention and hospitalisation. Monitoring the frequency and causes of these emergency admissions can help identify potential gaps in epilepsy management, including medication adherence, seizure control, and access to specialised care. It also highlights the need for effective education and support for families, caregivers, and healthcare professionals in managing epilepsy and preventing seizures. By analysing these admissions, healthcare providers and policymakers can work towards improving epilepsy care, reducing the occurrence of status epilepticus, and enhancing the overall well-being of children and young people with epilepsy.
Admissions for epilepsy (10-18 years)
This indicator covers emergency admissions for epilepsy among young people, presenting the crude rates per 100,000 population aged 10-18 years. The inclusion of this indicator is based on the age range's relevance to young people.
For the year 2021/22, the crude rate of emergency admissions for epilepsy among young people aged 10-18 years in Bury was 44.6 per 100,000 population, which is statistically similar to the England average of 56.4 (Child and Maternal Health, 2022).
Regarding inequalities, specific data for Bury are unavailable. However, data by sex for England reveals statistically higher admission rates for epilepsy among males (59.1 per 100,000) and statistically lower rates for females (85.4 per 100,000) when compared to overall England average. A slight deprivation gradient is observed by deprivation decile, with least deprived deciles (45.2) having the lowest emergency admission rates. Conversely, children in the most deprived decile (64.2) have the highest emergency admission rate (Child and Maternal Health, 2022).
Injuries
Injuries are a leading cause of hospitalisation and premature mortality in children and young people. They are also a source of long-term health problems, such as mental health issues related to the experience(s).
Examining hospital admissions caused by unintentional and deliberate injuries in young people is crucial for public health surveillance, injury prevention planning, resource allocation, policy development, and evaluation of interventions. Understanding the causes of hospital admissions helps shape child safety policies, ensures appropriate allocation of healthcare resources, and allows evaluation of preventive measures. This helps create safer environments for young people and promotes their overall well-being.
Hospital admissions caused by unintentional and deliberate injuries in young people aged 15-24 years
Data on hospital admissions for young people aged 15-24 due to unintentional and deliberate injuries are available in the form of a crude rate. This rate represents the number of admissions per 10,000 population in the same age group. Specifically, for Bury, in the period of 2021-22, the rate of hospital admissions caused by unintentional and deliberate injuries was 114.5 per 10,000 population 15-24 years of age. This rate is statistically similar to the national average of 118.6 for England. There are no trend data comparing these hospital admissions for both Bury and England (Child and Maternal Health, 2022).
In comparison to its six neighbouring statistical children services, Bury has the 4th highest rate of hospital admissions within this age range. The highest rate among Bury neighbours is observed in Sefton, with a rate of 164.3 per 10,000 population 15-24 years of age, while the lowest rate is in Calderdale, at 95.5 per 10,000 residents (Child and Maternal Health, 2022).
Data on inequalities in Bury are present by sex only. They indicate higher rates of hospital admissions in females (statistically significant), with a rate of 153.6 per 10,000 population 15-24 years of age. On the other hand, males in Bury have a rate of 82.8 per 10,000, which is statistically similar to the England average (Child and Maternal Health, 2022).
Data for England by Sex suggests a similar pattern with higher (statistically significant) hospital admissions rates in females of 125.8 per 10,000 residents 15-24 years of age, compared to males who have a rate of 111.4 per 10,000 (Child and Maternal Health, 2022).
Examining the data based on levels of deprivation, there is a reverse gradient by levels of deprivation. The highest rate of admissions are in the 3rd least (127.6) and least deprived decile (126.8) and the lowest rates are observed in the 2nd most (105.3) and least deprived decile, with a rate of 114.3 per 10,000 residents (Child and Maternal Health, 2022).
Mental Health
Understanding and addressing mental health in children is crucial for their overall well-being. Various risk factors, including adverse childhood experiences, family dynamics, socioeconomic factors, and access to mental health services, can impact children's mental well-being.
Hospital admissions for mental health conditions (<18 years of age)
One in ten children and young people aged 5-16 years has a clinically diagnosable mental health problem and, of adults with long-term mental health problems, half will have experienced their first symptoms before the age of 14. Self-harming and substance abuse are known to be much more common in children and young people with mental health disorders – with ten per cent of 15-16 year olds having self-harmed. Failure to treat mental health disorders in children and young people can have a devastating impact on their future, resulting in reduced job and life expectations.
Hospital admissions for mental health conditions are presented as crude inpatient admission rate for mental health disorders per 100,000 population aged 0-17 years. The crude rate in Bury for 2021/22 was at 91.4, similar to England’s average of 99.8 (Child and Maternal Health, 2022). There are no trend data available for Bury and England.
Bury has the 2nd lowest admission rates from its group of 6 children statistical neighbours with the highest rate in Stockton-on-Tees at 115.8 and lowest in Calderdale at 77.7 (Child and Maternal Health, 2022)
Data on inequalities in Bury are available by Sex only, with higher admission rates in Females (118.1 per 100,000 population aged 0-17 years) compared with Males (44.3 per 100,000 population aged 0-17 years) (Child and Maternal Health, 2022).
England data by Sex shows higher admission rates (statistically significant) in Females at 143.4 compared with Males at 58.1 (Child and Maternal Health, 2022). Examining data by deprivation for England shows increasing rates of hospital admissions for mental health conditions (<18 years) by decreasing levels of deprivation overall. The highest rate is in the second least deprived decile (119.9) followed by the least deprived decile (113.6) and the lowest rate (85.4) is in the most deprived decile for 2021/22 (Child and Maternal Health, 2022).
Hospital admissions as a result of self-harm (10-24 years)
Analysing data on hospital admissions for self-harm in young people is of utmost importance in this regard. By closely examining this data, valuable insights are gained into the prevalence, patterns, and severity of self-harm behaviours among young people. Hospital admissions for self-harm in young people have increased in recent years, with admissions for young women being much higher than admissions for young men. With links to other mental health conditions such as depression, the emotional causes of self-harm may require psychological assessment and treatment. This information helps identify high-risk groups, tailor interventions, and provide timely support and prevention strategies. Accurate and comprehensive data on hospital admissions for self-harm in children is essential for shaping effective mental health policies, improving service provision, and promoting the mental well-being of young people.
Data for this indicator are presented as directly standardised rate of finished admission episodes for self-harm per 100,000 population aged 10-24 years. Hospital admissions rate as a result of self-harm for Bury during the period 2021/22 was 408.3 per 100,000 population aged 10-24 years, statistically similar to England average of 427.3. There are no trend data comparing these hospital admissions for both Bury and England (Child and Maternal Health, 2022).
In comparison to its six neighbouring statistical children services, Bury has the 3rd highest rate of hospital admissions within this age range. The highest rate among Bury neighbours is observed in Sefton, with a rate of 695.5 per 100,000 population 10-24 years of age, while the lowest rate is in Calderdale, at 282.4 per 100,000 population (Child and Maternal Health, 2022).
Data on inequalities in Bury are present by sex only. They indicate significantly higher rates of hospital admissions in females (statistically significant), with a rate of 738.9 per 100,000. On the other hand, males in Bury have a rate of 103.9 per 100,000, which is statistically lower than the England average (Child and Maternal Health, 2022).
Data for England by Sex suggests a similar pattern with higher (statistically significant) hospital admissions rates in females of 711.4 per 100,000 compared to males who have a rate of 153.8 per 100,000 (Child and Maternal Health, 2022).
Generally, higher rates of hospital admissions related to self-harm among females reflects complex emotional and societal realities. Females often find themselves navigating a path that can lead to feelings of intense pressure or distress, sometimes culminating in acts of self-harm. Influences such as societal expectations around appearance and traditional roles can intensify this journey. It's worth noting that females also tend to experience certain mental health challenges, like anxiety and depression, at a higher rate. These conditions are known to increase vulnerability to self-harming behaviours. However, these numbers solely represent hospital admissions and don't necessarily encompass the full spectrum of individuals who self-harm. In fact, males might not always reach out for or receive the help they need as readily.
Examining the data based on levels of deprivation, the lowest rates of admission are in the most deprived decile (391.6) and the highest rate of admissions are in the 5th most deprived (508.7), the third less deprived (479.2) and the least deprived decile (462.4) (Child and Maternal Health, 2022).
Hospital admissions as a result of self-harm (10-14 years)
This indicator is presented as crude rate of finished admission episodes for self-harm per 100,000 population. Hospital admissions rate as a result of self-harm in 10-14 years for Bury for the period 2021/22 is 233.8 per 100,000 similar (statistically significant) to England average of 307.1 (Child and Maternal Health, 2022). There are no trend data for Bury and England as the trend data are being reviewed by ONS.
Bury has the 4th highest rate for admission episodes of self-harm in its group of 6 statistical children service neighbours with the highest rate in Sefton at 619.7 and lowest in Stockton-on-Tees at 153.1 (Child and Maternal Health, 2022).
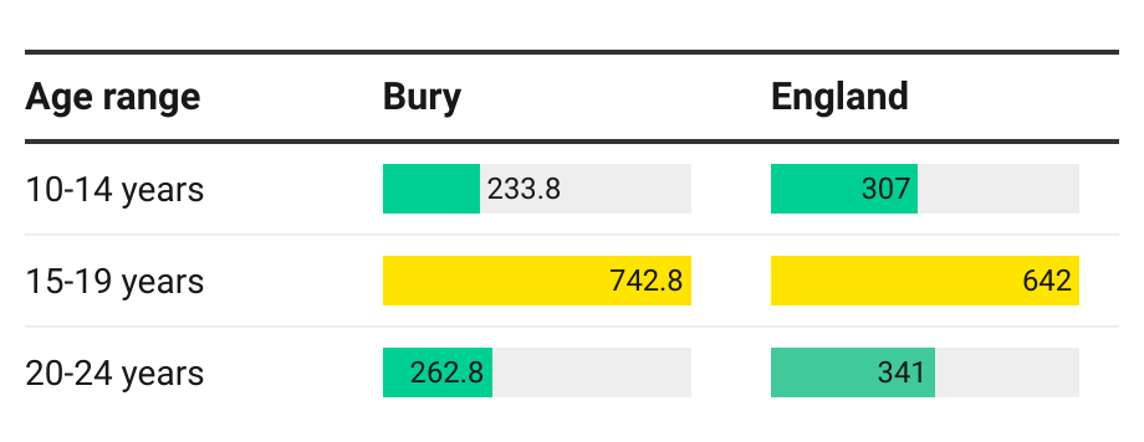
Data on inequalities for Bury are available by age, with lower rates in 10–14 year olds (233.8) and 20-24 year olds (262.8) and average rates (742.8) for 15-19 year olds. Examining data on inequalities for England, a similar pattern is seen by age with lower rates in 10-14 year olds (307) and 20-24 year olds (341) and average rates (642) in 15-19 year olds (Figure 5).
Figure 5: Inequalities in crude rates of finished admission episodes for self-harm per 100,000 population by age in Bury and England
Examining data by deprivation for England shows lower rates of self-harm in the most deprived deciles compared with the least deprived decile. The highest rate is in the fifth more deprived decile (364.6) followed by the fourth less (350.8) and third less (340.4) deprived decile and the lowest rate (270.9) is in the third most deprived decile for 2021/22 (Child and Maternal Health, 2022).
Hospital admissions as a result of self-harm (15-19 years)
This measure is presented as the crude rate of completed admissions for incidents of self-harm per 100,000 individuals in the population. The rate of hospital admissions resulting from self-inflicted harm among individuals aged 15-19 years in Bury during the period 2021/22 stands at 742.8 per 100,000 statistically similar to the average rate of 642 in England (Child and Maternal Health, 2022). Presently, there are lack of available data on trends for both Bury and England, as the data on trends is currently undergoing evaluation by the Office for National Statistics (ONS). Bury has the 2nd highest rate of admission episodes for self-harm in its group of 6 statistical children service neighbours with the highest rate in Sefton at 879.1 and lowest in Calderdale at 423 (Child and Maternal Health, 2022).
Data on inequalities for Bury are available by age and sex. For inequalities by age, please see Figure 9. Data by sex suggests a higher rate (statistically significant) of self-harm in females aged 15-19 years (1386.1) in Bury compared with males (165.8). Examining data on inequalities for England, a similar pattern is seen by sex with significantly higher rates in females (1088.3) compared with males (215.2) (Child and Maternal Health, 2022).
Examining data by deprivation for England shows increasing rates of self-harm by decreasing levels of deprivation overall. However, the highest rate is in the fifth more deprived decile (775.2) followed by the least deprived decile (749.6) and the lowest rate (562.9) is in in the most deprived decile for 2021/22 (Child and Maternal Health, 2022).
Substance Misuse
This section presents publicly available information on substance misuse, including alcohol, in young people in Bury. It is important to note that substance misuse goes beyond recreational drug use and includes alcohol consumption. There are indications that young individuals engaging in recreational drug use and excessive alcohol consumption face potential harm to their mental well-being, including the risk of suicide, depression, and disruptive behaviour disorders. Consistent usage of cannabis, other substances, and alcohol can also result in dependency. For individuals aged 10 to 15, an elevated probability of substance misuse, including alcohol, is associated with various negative encounters and behaviours, such as skipping school, being expelled, experiencing homelessness, being in foster care, and engaging in serious or frequent criminal activities.
Admission episodes for alcohol-specific conditions - Under 18s
The role of alcohol consumption in hospital admissions and mortality from various health conditions is noteworthy. Estimated annual expenditures stand around £3.5 billion for the NHS and £21 billion for society due to alcohol misuse. The government states that collective efforts are required to mitigate the excessive use of alcohol. In this context, this indicator serves as a pivotal strategy by the government and the Department of Health, to facilitate tangible, data-driven prevention activities at the local level. It aligns with the national goals outlined in the Government's Alcohol Strategy to decrease harm and is monitored through the Responsibility Deal Alcohol Network. Alcohol-related admissions can be curtailed via local strategies aimed at lessening alcohol misuse and related harm.
This indicator presents admissions to hospital for under 18s where the primary diagnosis or any of the secondary diagnoses are an alcohol-specific (wholly attributable) condition as crude rate per 100,000 population under 18 years of age. (OHID, 2022)
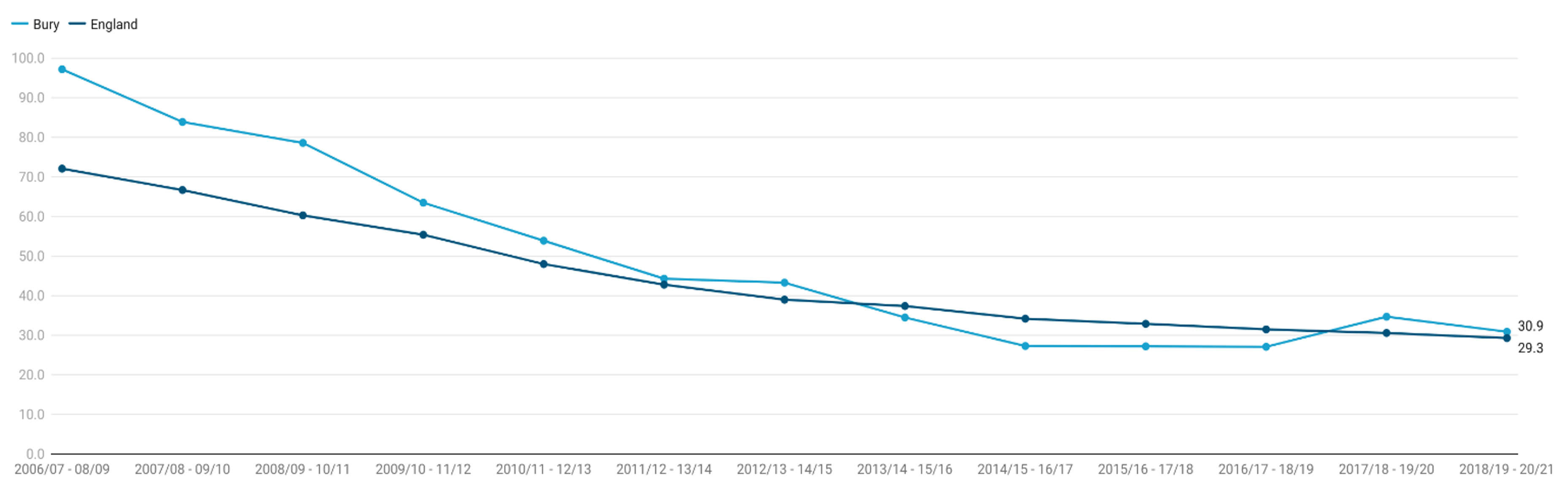
For the year period 2018/19-2020/21, the crude rate of admission episodes for alcohol-specific conditions for children and young people under 18 years of age in Bury was 30.9 per 100,000 population aged under 18 years, statistically similar to England average of 29.3 per 100,000 (Child and Maternal Health, 2021).
Examining trend for Bury, alcohol-specific admission rate steadily declined from the highest rate of 97.2 in 2006/07-2008/09 to 27.1 in 2016/17-2018-2019. This was followed by the first increase for over a decade in 2017/18-2019/20 to 34.7 before declining to 30.9 in the next period. The decline in Bury signals a reduction in alcohol-specific admissions in the area, suggesting possible successful interventions or changes in drinking behaviours amongst this age group.
England saw a consistent gradual decline, although at a less pronounced rate as Bury, from 72.1 in 2006/07-2008/09 to 29.3 in 2017/18-2019/20 (Child and Maternal Health, 2021).
Comparing Bury to England, Bury's rates were consistently higher until 2012/13 - 2014/15. Since then, the gap has narrowed, with Bury's rates descending more rapidly than England's. By the 2018/19 - 2020/21 period, the rates are almost identical, demonstrating that the interventions or societal changes in Bury have been effective in reducing their previously higher-than-average rates (Figure 6).
Such trends underscore the importance of continued, and potentially increased, efforts in alcohol education and preventative strategies within both the local and national contexts.
Figure 6: Trend in crude rates of Admission episodes for alcohol-specific conditions rate per 100,000 population under 18 years of age for Bury and England from the year 2008/09 to 2020/21
Bury has the 2nd lowest crude rates of admission episodes for alcohol-specific conditions rate per 100,000 population under 18 years of age in its group of 6 statistical children service neighbours with the highest rate in Sefton at 71 and lowest in Stockton-on-Tees at 22.8 (Child and Maternal Health, 2021).
Data on inequalities for Bury are available by sex only, with higher rates of admissions in females (31.9) compared with males (22.4). The rates in males and females are statistically similar to Bury average. Data by sex for England suggests that there are higher rates (36.1) of alcohol admissions in females compared with males (22.8). The rates in males are statistically lower and the rates in females are statistically higher than England average. Examining data by deprivation decile for alcohol-specific conditions admission rates in children under 18 years of age, the 5th more (32.4) and 2nd most deprived decile (31.2) in England has the highest rate and lowest rate of 25.6 is in the third more deprived decile for the period 2018/19-2020/21 (Child and Maternal Health, 2021).
Hospital admissions due to substance misuse (15 to 24 years)
This indicator presents directly standardised rate of hospital admission for substance misuse, per 100,000 population aged 15 to 24 years. (OHID, 2022)
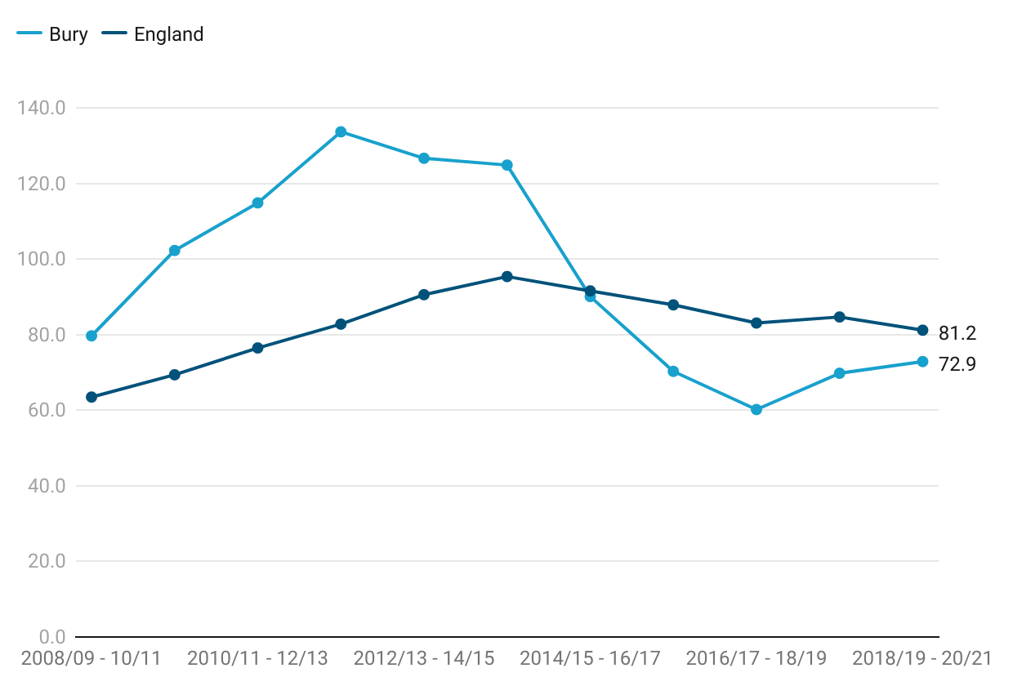
For the year period 2018/19-2020/21, the directly standardised rate of hospital admission for substance misuse, per 100,000 population aged 15 to 24 years in Bury was 72.9 per 100,000, statistically similar to England average of 81.2 per 100,000 (Child and Maternal Health, 2021).
Examining the trend in the directly standardised rate of hospital admission for substance misuse per 100,000 population aged 15 to 24 years in Bury from 2008/09 to 2020/21, the admission rate increased from 79.7 in 2008/09 – 10/11 and increased to a peak of 133.7 in 2011/12 - 13/14. This was followed by slight decline, with the rate reaching 90.1 in 2014/15 - 16/17. From 2015/16 to 2018/19, the rate remained relatively stable in Bury, ranging from 70.3 to 60.2. In the most recent data available for 2018/19 - 20/21, the rate in Bury was 72.9.
When examining the trend for England, the directly standardised rate of hospital admission for substance misuse among young people aged 15 to 24 years has shown fluctuations over the specified period. From 2008/09-10/11 the rate steadily increased from 63.5 to 95.4 in 2013/14-15/16. This was followed by a period of steady decline in the rate, reaching a low of 83.1 in 2016/17-18/19. In the most recent years, there has been a slight increase in the rate. From 2017/18 to 2019/20, the rate rose to 84.7, and in 2018/19-20/21, it increased further to 81.2 (Figure 7)
No recent trend for Bury could be calculated based on the five most recent data points.
Figure 7: Trend in directly standardised rate of hospital admission for substance misuse among young people aged 15 to 24 years for Bury and England from period 2018/19 to 2020/21
Bury has the lowest rate of hospital admission for substance misuse per 100,000 population aged 15 to 24 years in its group of 6 statistical children service neighbours with the highest rate in Sefton at 148.1 (Child and Maternal Health, 2021).
Data on inequalities for Bury are available by sex only, with higher rates of admissions in males (80.1) compared with females (65.1). The rates in males and females are statistically similar to Bury average. Data by sex for England suggests that there are slightly higher rates (81.6) of hospital admission for substance misuse in males (81.3) compared with females (80.3). The rates in males and females are statistically similar to England average. Examining data by deprivation decile for hospital admission for substance misuse, the rates of admission increase as the levels of deprivation increases. The highest rates of hospital admission for substance misuse per 100,000 population aged 15 to 24 years are in the most deprived decile at 137.4 and the lowest in the least deprived decile at 52.9.
Sexual and Reproductive Health
The term ‘sexual and reproductive health’ can be defined as a person’s right to a healthy body and the autonomy, education and healthcare to freely decide who to have sex with and how to avoid sexually transmitted infections or unintended pregnancy. Sexual health is an integral part of overall health and well-being, ensuring everyone can have pleasurable and safe sexual experiences, free of coercion, discrimination or health risks.
The Sexual and Reproductive Health Profiles have been developed by the UK Health Security Agency (UKHSA) and Office for Heath improvement & Disparities (OHID) to support local authorities, public health leads and other interested parties to monitor the sexual and reproductive health of their population and the contribution of local public health related systems.
Next, we present the indicators available in the profiles that are specifically relevant to the age group of young people.
Under 18 conception rates
Maternal age is an important factor for pregnancy outcomes. Younger women are at higher risk of adverse pregnancy outcomes. For example, they are less likely to take a folic acid supplement which protects against the risk of neural tube defects such as spina bifida (Bestwick et al, 2014). Babies born to women under the age of 20 are also approximately 20% more likely to be of low birthweight (ONS, 2023). Teenage mothers are less likely to complete their education, are more likely to raise their child alone and in poverty, and are at a greater risk for mental illness than their older counterparts. The infant mortality rate for babies born to teenage mothers is approximately 60% higher than that of babies born to older mothers. The children of teenage mothers are more likely to live in poverty and substandard housing, and to experience accidents and behavioural issues. Raising a child as a teenager is difficult and frequently results in negative outcomes for the baby's health, the mother's emotional health and well-being, and the likelihood of both parent and child living in long-term poverty (OHID, 2023).
Under 18 conception rate is measured as conceptions in women aged under 18 per 1,000 females aged 15-17 years. The rate for Bury in the year 2021 was 14.4 per 1000 females aged 15-17 years statistically similar to England average of 13.1 (Sexual and Reproductive Health Profiles, 2021). No trend data are available for Bury and England.
Compared to Bury 16 statistical neighbours, Bury has the 10th highest under-18 conception rate, with the highest rate in St. Helens at 25.9 and lowest in Swindon at 9 (Sexual and Reproductive Health Profiles, 2021). There are no data on inequalities at Bury level but England data suggests increasing conception rates with increasing levels of deprivation. The most deprived decile in England has an under-18 conception rate of 18.2 compared with 6.8 in the least deprived decile for the year 2021 (Sexual and Reproductive Health Profiles, 2021).
Under 18 conceptions leading to abortion
It is increasingly common for pregnant young women under 18 to have an abortion. Access to family planning and sexual health services, and the availability of independent sector abortion provision, directly affect abortion proportions. More deprived areas in England have both higher conception rates and a lower proportion of under-18 pregnancies ending in abortion.
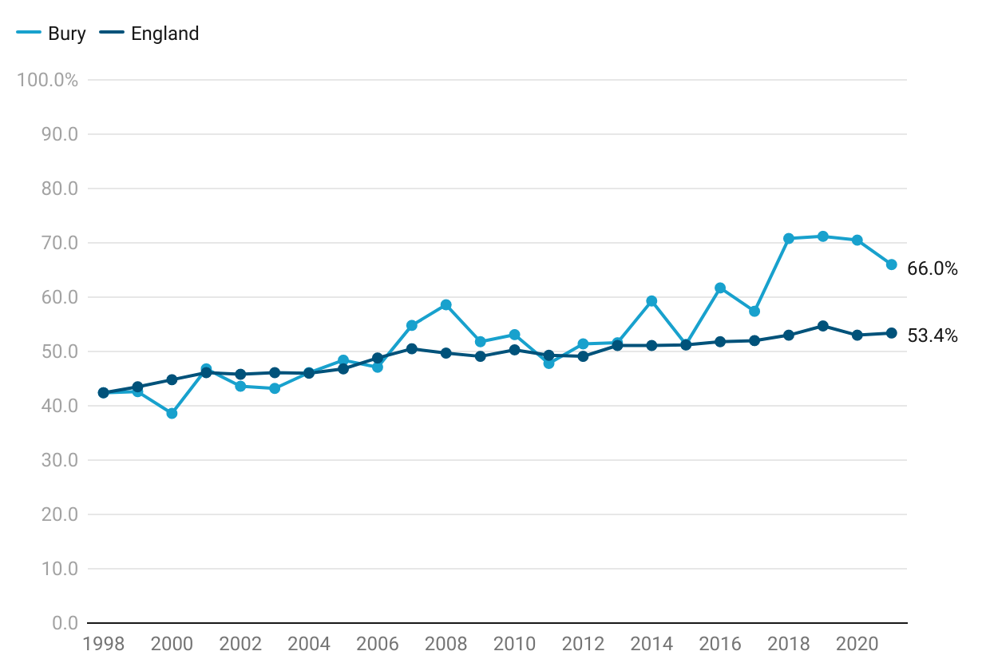
Most recent data for Bury shows that 66% of under 18 conceptions led to abortion, higher (not statistically significant) than England average of 53.4%. Figure 8 presents the percentage of conceptions to those aged under 18 years that led to an abortion in Bury and England from the year 1998 to 2010. The percentage of abortions in Bury ranged from 38.6% in 2000 to 71.2% in 2019. From the year 1998 to 2000, there was a decrease in the percentage of abortions from 42.4% to 38.6% and then started to increase again. From the year 2001, the percentage of under 18 conceptions leading to abortion continued to increase from 46.8% to reach a peak of 71.2% in 2019, before declining to 70.5% in 2020 and 66% in 2021. The large fluctuation in data for Bury may be due to small numbers at the local level.
The trend in England is different from that observed in Bury with less fluctuation in the data ranging from 42.4% to 53% from 1998 to 2020. The percentage of abortions in under-18s increased steadily from 42.4% in 1998 to 50.5% in 2007, remaining stable until 2012 at 49.1% before steadily increasing to the peak in 2019 at 54.7% and slightly declining to 53.4% in 2021 (Figure 8). There is no significant trend in Bury based on the 5 most recent data points.
Figure 8: Comparison of percentage (%) of under 18 conceptions leading to abortions for the years 1998 to 2021 for Bury and England
Bury has the 4th highest under 18 conceptions leading to abortion in its group of 16 similar local authorities with the highest percentage in Stockport at 71.2% and lowest percentage in Derby at 27.3% (Sexual and Reproductive Health Profiles, 2021). There are no data on inequalities within Bury but England data suggests decreasing percentage of under 18 conceptions leading to abortion with increasing levels of deprivation. The most deprived decile in England has an under-18 abortion percentage of 46.6% compared with 61.7% in the least deprived decile for the year 2021 (Sexual and Reproductive Health Profiles, 2021).
Teenage mothers
Bury has the 4th highest under 18 conceptions leading to abortion in its group of 16 similar local authorities (Child and Maternal Health, 2022).
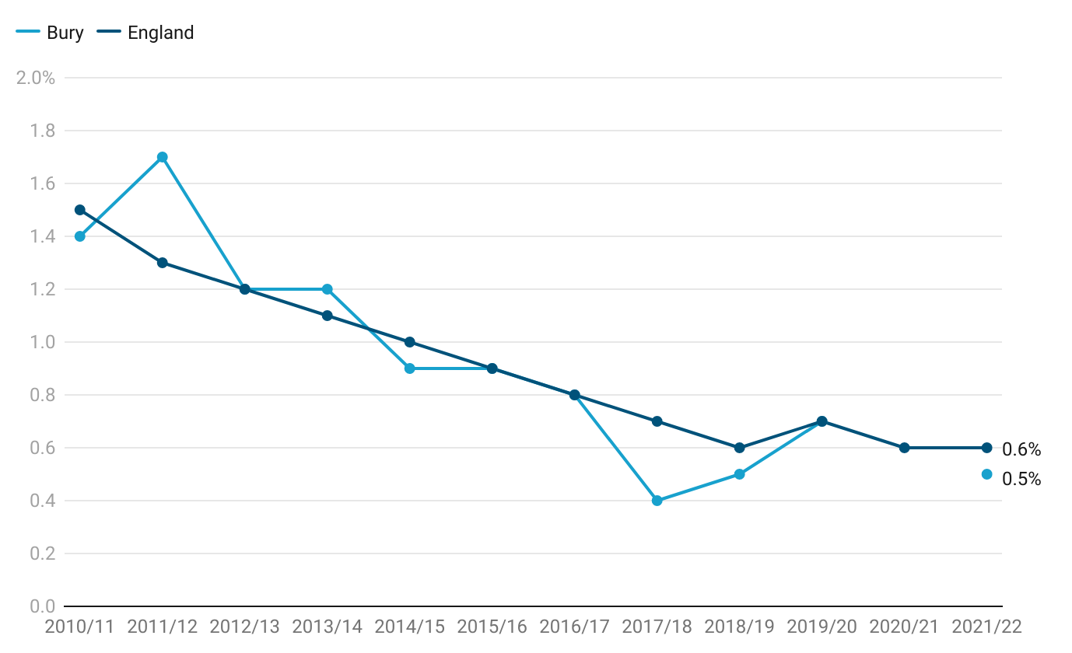
In Bury, the trend in teenage mothers (%) has shown a declining pattern from 2010/11 to 2017/18, with the rate decreasing from 1.40% to 0.40%. However, from 2018/19, there has been a slight increase in the rate, reaching 0.70% in 2019/20. It is important to note that no data are available for Bury for the year 2020/21, possibly due to the suppression of small numbers. The most recent data available for 2021/22 shows a slight decline to 0.50%.
The trend in teenage mothers (%) in England has also followed a similar pattern, with a decline from 1.50% in 2010/11 to 0.70% in 2020/21. The rate remained relatively stable from 2017/18 to 2019/20, with slight fluctuations within the range of 0.60% to 0.70% (Figure 9).
Trend data based on most recent data points in Bury shows no significant trend.
Figure 9: Comparison of percentage (%) of births to teenage mothers for the period 2010/11 to 2021/22 for Bury and England
Bury has the lowest percentage of teenage mothers in its group of 6 statistical children service neighbours with the highest percentage in Stockton-on-Tees at 1.3% (Child and Maternal Health, 2022). There are no data on inequalities within Bury but England data suggests increasing percentage of teenage mothers with increasing levels of deprivation. The most deprived decile in England has percentage of teenage mothers at 1.3% (statistically worse than England average) compared with 0.1% in the least deprived decile for the year 2021 (Child and Maternal Health, 2022). Data by ethnic groups suggest highest proportion of teenage mothers in the mixed/multiple ethnic groups (0.8%) and White (0.7%) ethnic groups and lowest in the Asian/Asian British including Chinese (0%).
Chlamydia
Chlamydia is the most commonly diagnosed bacterial sexually transmitted infection in England, particularly affecting young adults more than any other age group. It poses risks to sexual and reproductive health, including acute infections with symptoms and complications such as pelvic inflammatory disease (PID), ectopic pregnancy, and infertility.
The National Chlamydia Screening Programme (NCSP) plays a crucial role in promoting opportunistic screening for sexually active individuals under 25 years old. In June 2021, changes to the program were implemented to prioritise reducing the reproductive harm caused by untreated infections, with a specific focus on offering screening to young women under 25 years old.
The chlamydia detection rate among individuals under 25 years old serves as a measure of chlamydia control efforts, aiming to decrease the incidence of reproductive complications associated with chlamydia and interrupting its transmission. A higher detection rate indicates increased control activities, although it does not directly measure morbidity. The inclusion of this indicator in the Public Health Outcomes Framework (PHOF) enables monitoring of progress in controlling chlamydia and ensuring the delivery of accessible and high-volume chlamydia screening services. It serves as a tool to assess the effectiveness of chlamydia control strategies and their impact on public health outcomes.
Chlamydia detection rate per 100,000 aged 15 to 24 (persons)
This indicator is defined as all chlamydia diagnoses in 15 to 24 year olds attending sexual health services (SHSs) and community-based settings, who are residents in England, expressed as a crude rate per 100,000 population. Data excludes people accessing services located in England who are residents in Wales, Scotland, Northern Ireland or abroad. The England total includes tests which did not have sufficient location information to be attributed to a local authority of residence.
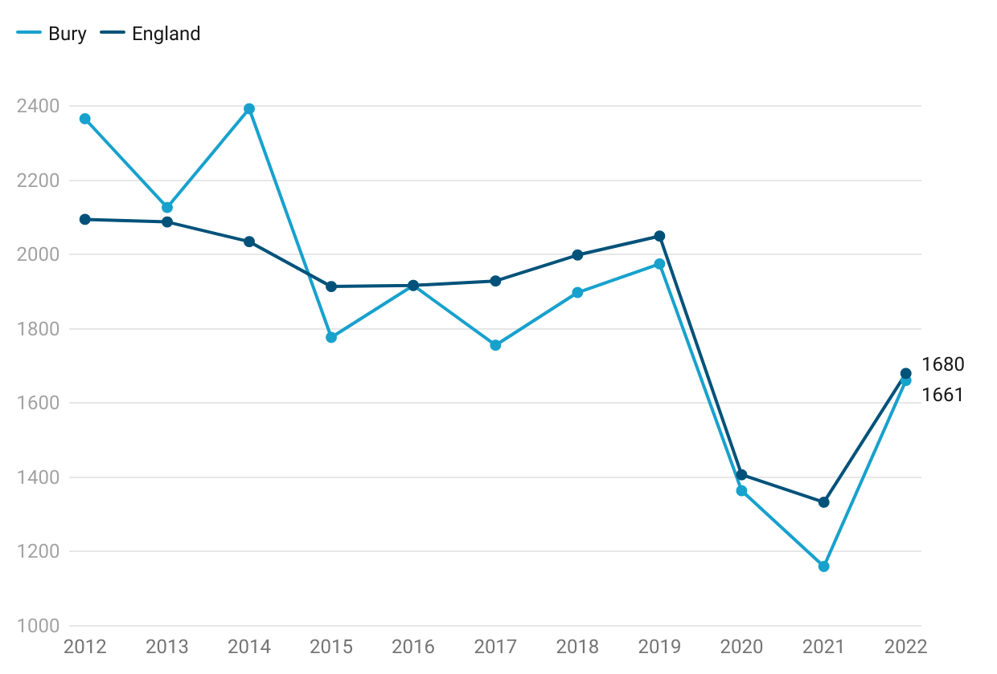
Chlamydia detection rate in young people aged 15-24 in Bury for the year 2022 was 1,661 per 100,000 population aged 15-24 years, similar to England average of 1,680 per 100,000. In Bury, the trend for Chlamydia detection crude rates per 100,000 population aged 15 to 24 has shown a consistent decline from 2012 to 2022. The rates started at 2,366 in 2012 and gradually decreased to 1,160 in 2021. However, there was a slight increase to 1,661 in 2022. Bury has experienced a decreasing trend in Chlamydia detection rates based on the 5 most recent data points.
The trend in Chlamydia detection crude rates per 100,000 population aged 15 to 24 in England has also demonstrated a consistent decline over the specified period. The rates started at 2,095 in 2012 and steadily declined to 1,333 in 2021. However, there was a slight increase to 1,680 in 2022 (Figure 10).
Figure 10: Comparison of Chlamydia detection rate in young people aged 15-24 presented as crude rate per 100,000 population aged 15-24 years for the period 2012 to 2022 for Bury and England
Bury has the 7th highest Chlamydia detection rate in its group of 16 similar local authorities with the highest rate in Wigan at 2,227 per 100,000 and lowest rate in Dudley at 828 per 100,000 (Sexual and Reproductive Health Profiles, 2022). Detailed information on inequalities is available by sex only for Bury and will be presented later. England data suggests increasing chlamydia detection rate with increasing levels of deprivation. The highest detection rates are in 2nd (2,064), 3rd (1,941) and most deprived decile (1,922) decile in England and the lowest rates are in second least (1,240) and least deprived (1,026) deprived decile (Sexual and Reproductive Health Profiles, 2022).
Chlamydia detection rate per 100,000 aged 15 to 24 (female)
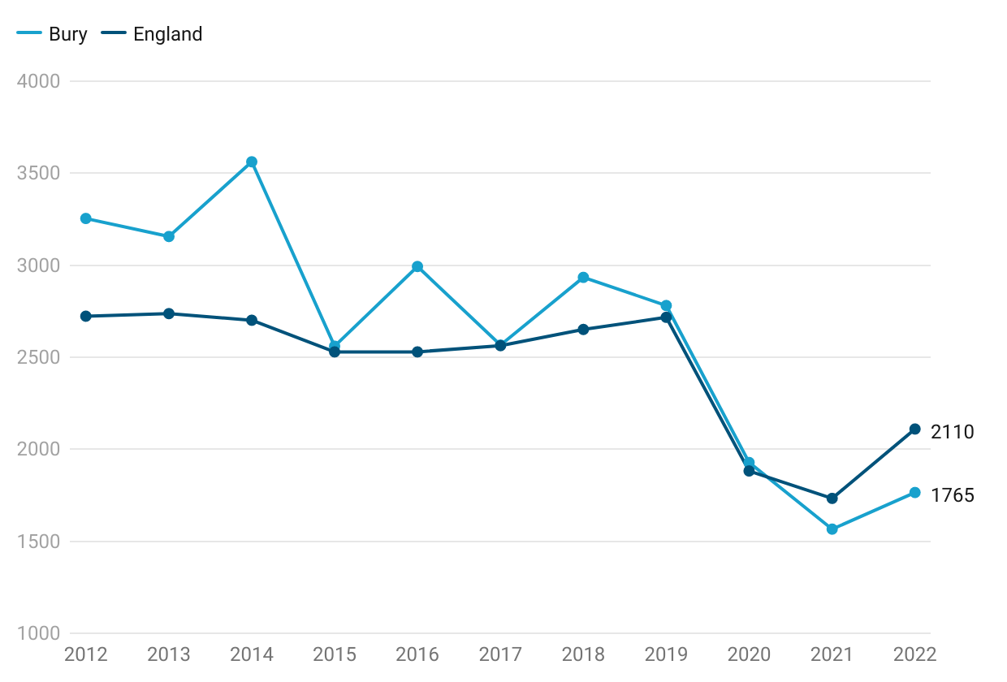
In Bury, the Chlamydia detection rate per 100,000 population aged 15 to 24 (female) in 2022 was 1,765, which was lower than the benchmark goal of ≥3,250 and lower than the England average of 2,110. The trend for Chlamydia detection crude rates per 100,000 population aged 15 to 24 (female) in Bury has consistently declined from 2012 to 2022. Starting at 3,254 in 2012, the rates gradually decreased to 1,566 in 2021. However, there was a slight increase to 1,765 in 2022. Based on the five most recent data points, Bury has shown a decreasing trend in Chlamydia detection rates.
Similarly, in England, the trend in Chlamydia detection crude rates per 100,000 population aged 15 to 24 (female) has also demonstrated a consistent decline over the specified period. Starting at 2,723 in 2012, the rates steadily declined to 1,733 in 2021. However, there was a slight increase to 2,110 in 2022 (Figure 11).
Figure 11: Comparison of Chlamydia detection rate in young people aged 15-24 (female) presented as crude rate per 100,000 population aged 15-24 years for the period 2012 to 2022 for Bury and England
Among its group of 16 similar local authorities, Bury has the 5th lowest Chlamydia detection rate per 100,000 population aged 15 to 24 (female). The highest rate within this group is observed in Wigan at 2,926 per 100,000, while the lowest rate is seen in Dudley at 1,115 per 100,000 (Sexual and Reproductive Health Profiles, 2022). No data on inequalities are present for Bury. England data suggests increasing chlamydia detection rate with increasing levels of deprivation. The highest detection rates are in 2nd (2,580) and most deprived decile (2,468) in England and the lowest rates are in second least (1,505) and least deprived (1,312) decile (Sexual and Reproductive Health Profiles, 2022).
Chlamydia detection rate per 100,000 aged 15 to 24 (Male)
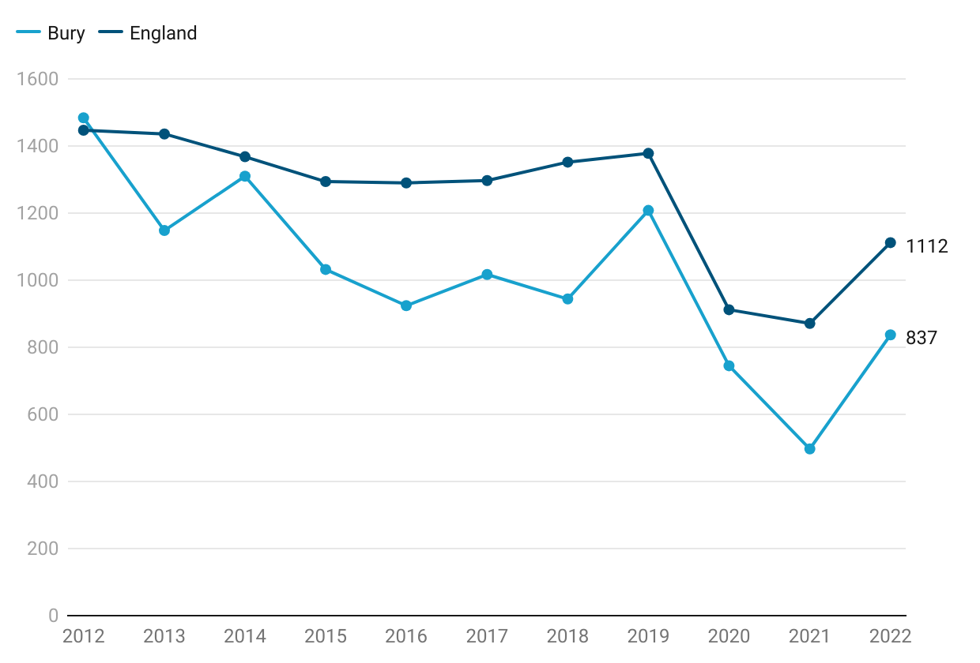
Chlamydia detection rate per 100,000 aged 15 to 24 (male) in Bury for the year 2022 was 837 per 100,000 population aged 15-24 years, lower than England average of 1,112 per 100,000. The trend for Chlamydia detection crude rates per 100,000 population aged 15 to 24 (male) has shown a consistent decline with slight fluctuations from 2012 to 2022. The rates gradually declined from 1,484 in 2012 to 497 in 2021. However, there was a slight increase to 837 in 2022. Bury has experienced a decreasing trend in Chlamydia detection rates based on the 5 most recent data points.
The trend in Chlamydia detection crude rates per 100,000 population aged 15 to 24 (male) in England has also demonstrated a consistent decline over the specified period. The rates started at 1,447 in 2012 and steadily declined with some fluctuations to 871 in 2021. However, there was a slight increase to 1,112 in 2022 (Figure 12).
Figure 12: Comparison of Chlamydia detection rate in young people aged 15-24 (male) presented as crude rate per 100,000 population aged 15-24 years for the period 2012 to 2022 for Bury and England
Among its group of 16 similar local authorities, Bury has the 5th lowest Chlamydia detection rate per 100,000 population aged 15 to 24 (male). The highest rate within this group is observed in Wigan at 1,518 per 100,000, while the lowest rate is seen in Dudley at 522 per 100,000 (Sexual and Reproductive Health Profiles, 2022). No data on inequalities are present for Bury. England data suggests increasing chlamydia detection rate with increasing levels of deprivation. The highest detection rates are in 2nd (1,378) and most deprived decile (1,248) in England and the lowest rates are in second least (809) and least deprived (700) decile (Sexual and Reproductive Health Profiles, 2022).