Mental health and illness
Good mental health means being generally able to think, feel, and react in the ways that you need and want to live your life, and being able to cope with day-to-day stresses. But if you go through a period of poor mental health you might find the ways you're frequently thinking, feeling or reacting become difficult, or even impossible, to cope with. This can feel just as bad as a physical illness, or even worse (Mind).
One in four adults and one in ten children experience mental illness, and many more of us know and care for people who do (NHS England). People in all walks of life can be affected by mental illness and at any point in their lives. Mental health problems represent the largest single cause of disability in the UK (NHS England) and are the second most important cause of disability for people living in Bury (Global Burden of Disease, 2021). In England in 2022, mental health conditions accounted for 18.5 million lost days of work, 10% of all lost days (Office for National Statistics, 2022).
Self-reported wellbeing
Subjective wellbeing is a broad measure of mental health. It tries to measure how happy or anxious people feel day-to-day as well as how satisfied they are with their lives overall. Improving subjective wellbeing has been a focus of government policy both in the UK and in several other countries.
The Office for National Statistics uses four questions to measure subjective wellbeing:
- Overall, how satisfied are you with your life nowadays?
- Overall, how happy did you feel yesterday?
- Overall, how anxious did you feel yesterday?
- Overall, to what extent do you feel the things you do in your life are worthwhile?
Responses are given on a scale of 0 to 10 (where 0 is “not at all satisfied or happy or anxious or worthwhile” and 10 is “completely satisfied or happy or anxious or worthwhile”). These questions are included in regular surveys.
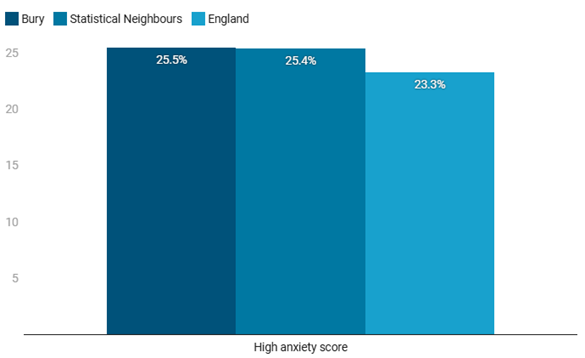
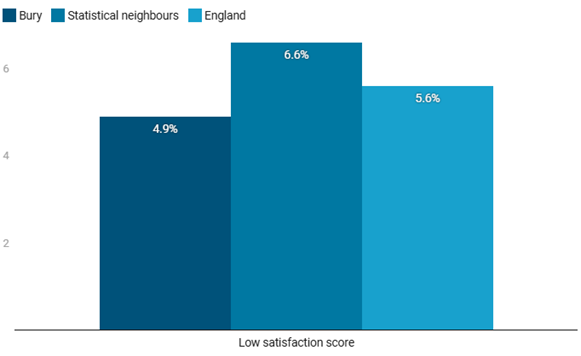
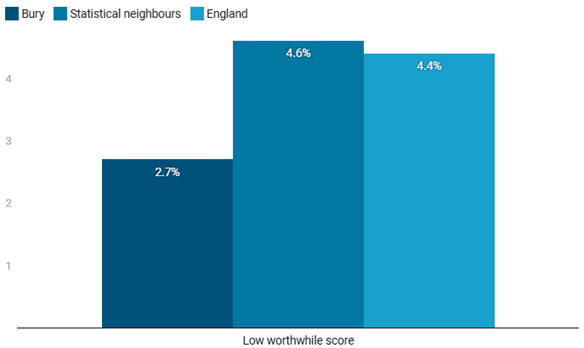
Figure 1 shows the percentage of people reporting high levels of anxiety (scores of 6-10), or low levels of happiness, life satisfaction, or feeling that the things they do are worthwhile (scores of 0-4) for 2022/23. This gives a high-level view of mental wellbeing of the population of Bury compared to statistically similar areas, and to England as a whole. The differences in the data are not statistically significant, suggesting that they could be consistent with a similar underlying level of mental wellbeing, with the exception of the percentage of people with a low worthwhile score, as Bury is significantly better than England in this measure for 2022/23.
Because the data are based on surveys, we do not have data for smaller areas or for different sections of Bury’s population that would enable us to assess inequalities in subjective wellbeing.
Figure 1: Subjective Wellbeing Proportion - %, Bury, statistical neighbours and England, 2022/23 (Public Health Outcomes Framework, 2023)

Prevalence of common mental illness
Nearly one in six adults (16.3%) in Bury are recorded on GP practice registers with a diagnosis of depression for 2022/23 (Public Health Profiles, 2023). Figure 2 below shows prevalence (the proportion of people aged 18 and over with depression, as recorded on practice disease registers) for Bury Local Authority. These data show that although it was the same figure in Bury as it was for England for 2021/22, the figure for Bury has increased further for 2022/23 and is now significantly above the rate for England. There has been an increasing trend for both Bury and England. Bury previously had lower rates of diagnosed depression than England, but caught up sharply in 2021/22. Bury has the seventh highest rates of prevalence of depression for those aged 18 and above when compared to statistical neighbours (Public Health Profiles, 2023). It is important to note that diagnosed prevalence data depend on access to care and the likelihood of getting a diagnosis if a person has the condition as well as the prevalence of the condition in the population. Based on the data below we cannot rule out improvements in diagnosis, rather than increases in disease prevalence as an explanation for the increasing rates of diagnosed depression.
Figure 2: Depression: QOF prevalence (18+ years) (%), Bury and England, 2013/14 – 2022/23 (Public Health Profiles, 2023)

Figure 3 below shows yearly incidence (the proportion of people who develop the condition in a year) for Bury Integrated Care Board (ICB). Having initially been lower than England from 2013/14 to 2020/21, there was a significant increase in Bury ICB from 2021/22, leaving the rate now significantly higher than that in England. The rate in Bury ICB (2.1%) for 2023/24 is similar to the rate for Greater Manchester ICB (2.2%) (Public Health Profiles, 2024).
Figure 3: Depression: QOF incidence – new diagnosis (18+ years) (%), Bury ICB and England, 2013/14 – 2023/24 (Public Health Profiles, 2024)

Survey data make it possible to try to measure prevalence of mental illness directly, without relying on people getting a diagnosis. According to estimates for 2016/17 (the last year for which data are available), Bury has significantly higher depression and anxiety prevalence compared with England. 15.3% of people aged 18 and over in Bury reported they were anxious or depressed in the GP Patient Survey in 2016/17, compared to 13.7% in England and 15% on average for Bury’s statistical neighbours.
Figure 4 below illustrates that with the exception of a slight decrease in 2015/16, Bury has shown an increasing trend since 2013/14 consistent with the trend seen nationally (Public Health Profiles).
Figure 4: Depression and anxiety prevalence (GP Patient Survey): % of respondents aged 18+, Bury and England, 2013/14 – 2016/17

Approximately 2,120 people (1.01% of the population) in Bury are recorded as having a mental health disorder including schizophrenia, bipolar affective disorder and other psychoses as recorded on practice disease registers. This is similar to the percentage recorded in England (0.95%) and the average across Bury’s statistical neighbours (0.96%) (Public Health Profiles).
Mental health harms
Children and young people
Mental health is as important to a child's safety and wellbeing as their physical health. It can impact on all aspects of their life, including their educational attainment, relationships and physical wellbeing. Mental health can also change over time, to varying degrees of seriousness, and for different reasons (NSPCC).
One in ten children aged 5-16 years has a clinically diagnosable mental health problem and, of adults with long-term mental health problems, half will have experienced their first symptoms before the age of 14. Bury is not significantly different to England for hospital admissions for mental health conditions for those aged under 18 years (Public Health Profiles).
Table 1: Hospital admissions for mental health conditions (<18 yrs) Crude rate – per 100,000, Bury and England, 2023/24
| Bury | England | |
| 2023/24 | 68.2 | 80.2 |
The National Clinical Practice Guidelines published by the British Psychological Society state that children with learning or physical disabilities have a risk of developing a mental health problem compared to the national population (Public Health Profiles).
Bury remains significantly worse than England for the percentage of school pupils with Special Education Needs (SEN) who are identified as having social, emotional and mental health needs. Bury is the fourth highest amongst its statistical neighbours for this measure, and is reflecting the national trend of increasing and getting worse (Public Health Profiles). Figure 5 below illustrates the trend for Bury and England for this measure
Figure 5: School pupils with social, emotional and mental health needs: % of school pupils with social, emotional and mental health needs, Bury and England, for 2017/18 to 2022/23

Impacts on adult life
Poor mental health can create a negative feedback loop, where poor mental health causes worse access to basic building blocks of health, such as employment or housing, or affects behavioural causes of health such as smoking or drug and alcohol use, which then in turn worsen physical and mental health.
The proportion of people in Bury who are in contact with secondary mental health services who live in stable accommodation (53%) is significantly worse than England (57.7%) and statistically similar areas. The gap in employment rate between working age adults in contact with secondary mental health services and other adults is similar in Bury (68.8%) compared with England (66.5%) and statistically similar areas (66%). Bury is however the third highest amongst its fifteen statistical neighbours in this measure (Public Health Profiles).
Figure 6: employment and housing for people in contact with secondary mental health service, 2020/21

Smoking
Smoking is an important contributor to the gap in life expectancy between people with mental illnesses and others. The smoking rate among people with long-term mental illness fell in Bury from 37.9% in 2013/14 to 20.6% in 2022/23. This took Bury from comparable to the national average to being significantly lower than the average for England and of statistically similar areas.
Figure 7: Smoking prevalence (%) among adults with a long-term mental illness, Bury, statistical neighbours, and England, 2013/14 to 2022/23

Self-harm
Self-harm is an important manifestation of poor health and a significant risk factor for suicide. Although self-harm can affect people of all ages, it is more common in children and young people – with 10% of 15-16 year olds nationally having self-harmed. Rates of hospital admission for self-harm are higher for females than for males.
The rate of hospital admissions for intentional self-harm in Bury is statistically similar to that in England as a whole. Figure 8 below shows age-standardised hospital admission rates for both sexes combined for Bury and England.
Figure 8: Emergency Hospital Admissions for Intentional Self-Harm, Directly standardised rate – per 100,000, Bury, and England, 2023/24

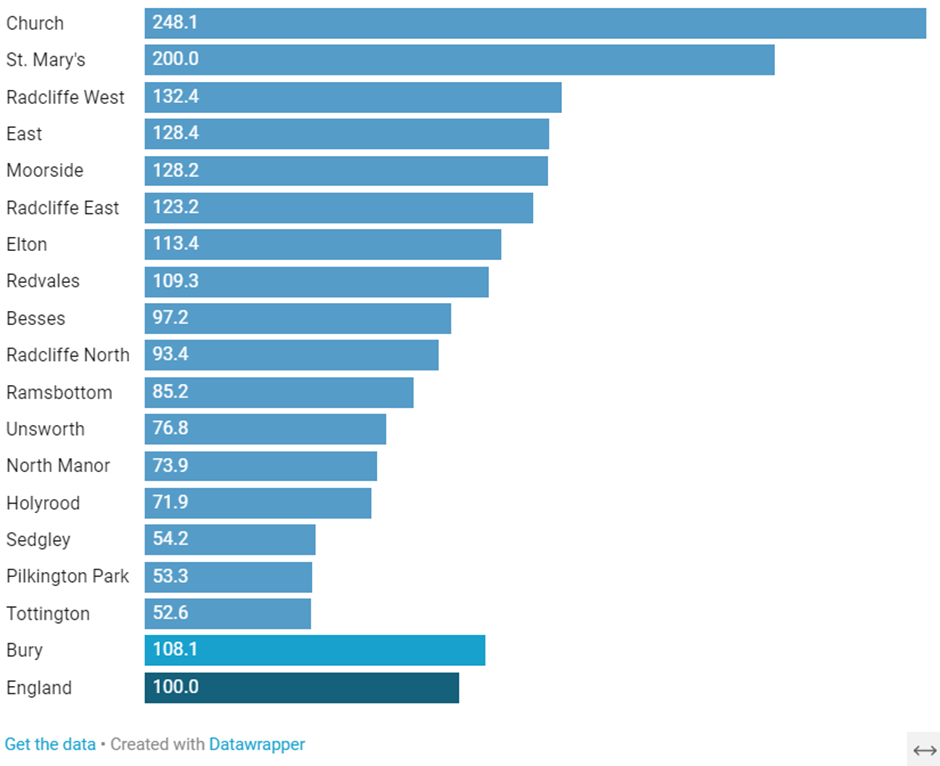
Geographical variations exist within Bury, as illustrated in Figure 9 below. Data are available only for the period 2016/17-2020/21. Church ward within Bury has the highest rate of emergency hospital admission rate for intentional self-harm, whereas Tottington has the lowest rate.
Figure 9: Emergency hospital admissions for intentional self-harm, standardised admission ratio. Indirectly standardised ratio – per 100, Wards in Bury, 2016/17 – 2020/21
2020/21
Mortality
Premature mortality in people with mental illness
People who experience severe mental illnesses die younger on average than other people. This is caused by a combination of factors already discussed as well as increased risk of suicide.
These inequalities are significantly worse in Bury than the average for statistically similar areas or England. Figure 10 shows directly age standardised rate of deaths of adults, aged 18 - 74, with SMI, per 100,000 population. SMI is defined as having a referral to mental health services in the five years preceding death (Public Health Profiles). There has been an increase in excess mortality across England as a whole over the time for which data are available. However, Bury has remained significantly worse than England in this measure across the last data point. Excess mortality affects both males and females with severe mental illness, although excess mortality is higher in males.
Figure 10: Premature mortality in adults with severe mental illness (SMI) for females, males, and both sexes combined, Directly standardised rate – per 100,000, Bury and England, 2015-17 – 2021-23

Suicide
Suicide is a significant cause of death and is an indicator of underlying rates of mental ill-health. Suicide rates tend to be highest among working-age adults, especially in men.
The suicide rate in Bury (13.6 per 100,000 population) is statistically similar to the rate for England (10.7 per 100,000 population) for 2021-23 (Public Health Profiles). The rate has increased since 2017-19, although the rate in Bury remains statistically similar to the England average. Bury has the 3rd highest suicide rate when compared to its 15 other statistical neighbours.
Figure 11: Suicide rate, Directly standardised rate – per 100,000 in Bury, 2016-18 to 2021-23

The suicide rate is significantly higher in males (20.6) in Bury than females (6.7), reflecting the national and regional trends.
Support for mental health problems
Psychological therapies have been shown to improve outcomes for people with mental health problems. Data for Bury Clinical Commissioning Group (CCG) in September 2019 show that 23.7% of those estimated to have anxiety/depression entered IAPT (Improving Access to Psychological Therapies) that month. (Although CCGs ceased to exist in July 2022 when they transitioned to Integrated Care Systems (ICS), CCG is still referred to as the data from the specified time period was when CCGs were still in existence.) This is significantly better than the England average (18.3%) and second highest amongst all CCGs in Greater Manchester. Access to IAPT services in Bury CCG increased significantly from August 2019 (Public Health Profiles). Furthermore, the percentage of people aged 18+ who completed IAPT treatment who are “moving to recovery” was 58% for Bury CCG in September 2019, higher than the England figure of 51.9% (Public Health Profiles).
Bury CCG is significantly worse than England for the percentage of newly diagnosed patients with depression who had a review 10-56 days after diagnosis (denominator incl. PCAs), with Bury being the worst performing CCG in England 2021/22. The rationale for such follow-up measurement is derived from the recognition that depression is often a chronic disease, yet treatment is often episodic and short-lived. If treatment with antidepressants is initiated, patients should be followed-up regularly for several months. Figure 13 below illustrates that prior to 2020/21 Bury CCG was significantly better than England, yet since then Bury has seen a precipitous decline in this measure (Public Health Profiles).
Figure 13: Newly diagnosed patients with depression who had a review 10-56 days after diagnosis (%), Bury CCG, Greater Manchester, and England, 2017/18 to 2021/22

Services
There are lots of services that offer mental health support, which can be found through the Health and Wellbeing Digital Hub on The Bury Directory.
Support for Adults includes links to relevant services and helpful documents which can be downloaded. The Support for Children and Young People page on The Bury Directory contains links to resources for topic specific services such as anxiety, eating disorder support and emotionally based school avoidance, as well as links to other relevant services.